This article contains Operative Note Templates to be used while charting procedures. Below are approximately 40 templates corresponding to the most common aesthetic procedures.
IMPORTANT: To have any of these templates moved into your practice account, email support@remedly.com with the name of the template(s) you would like, and a member of our team will move them into your account for you.
You can further customize these templates once we have moved them into your account. Click on the desired template name below to view details.
Table of Contents:
Botox/Dysport/Jeaveau Treatment
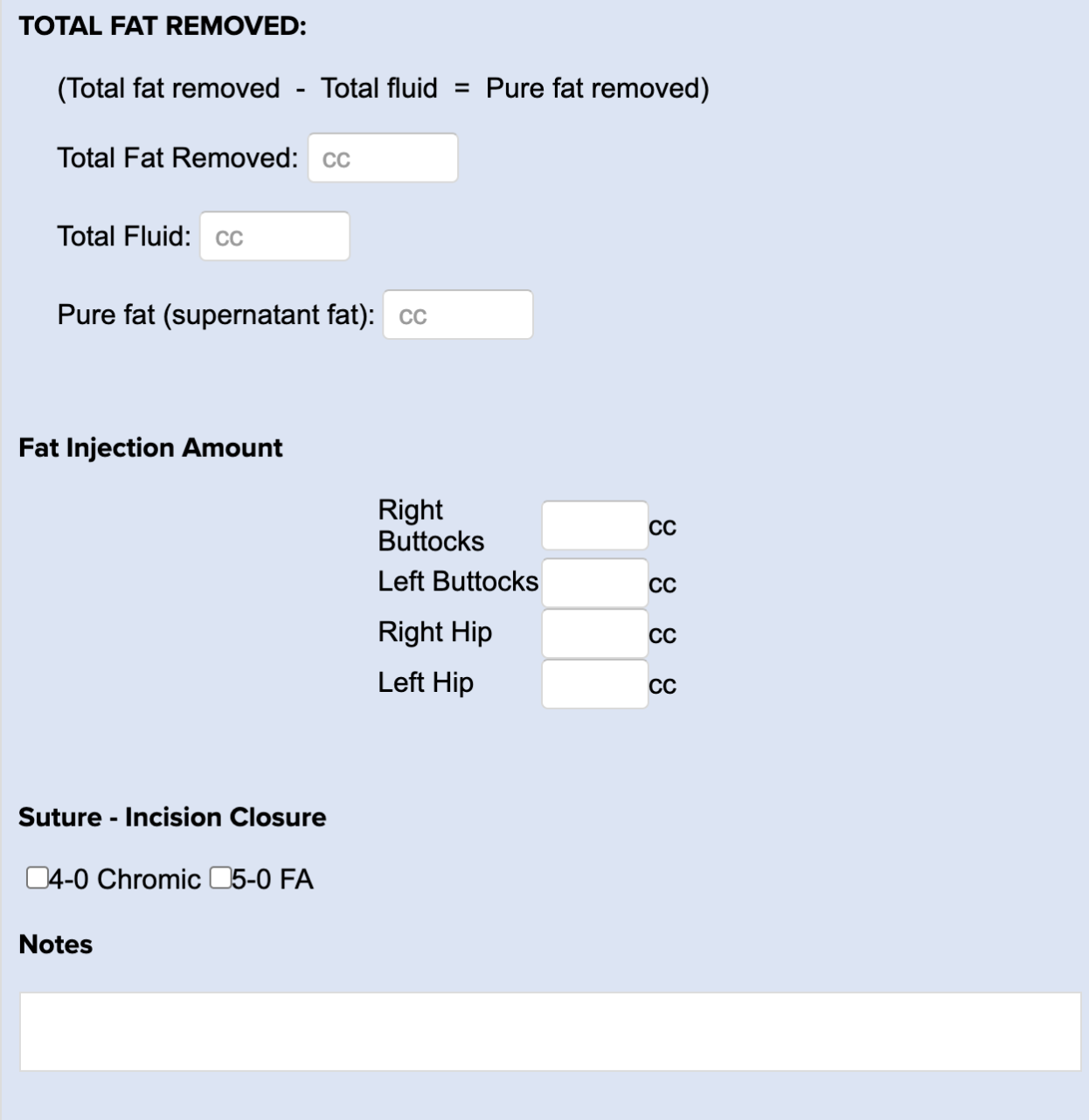
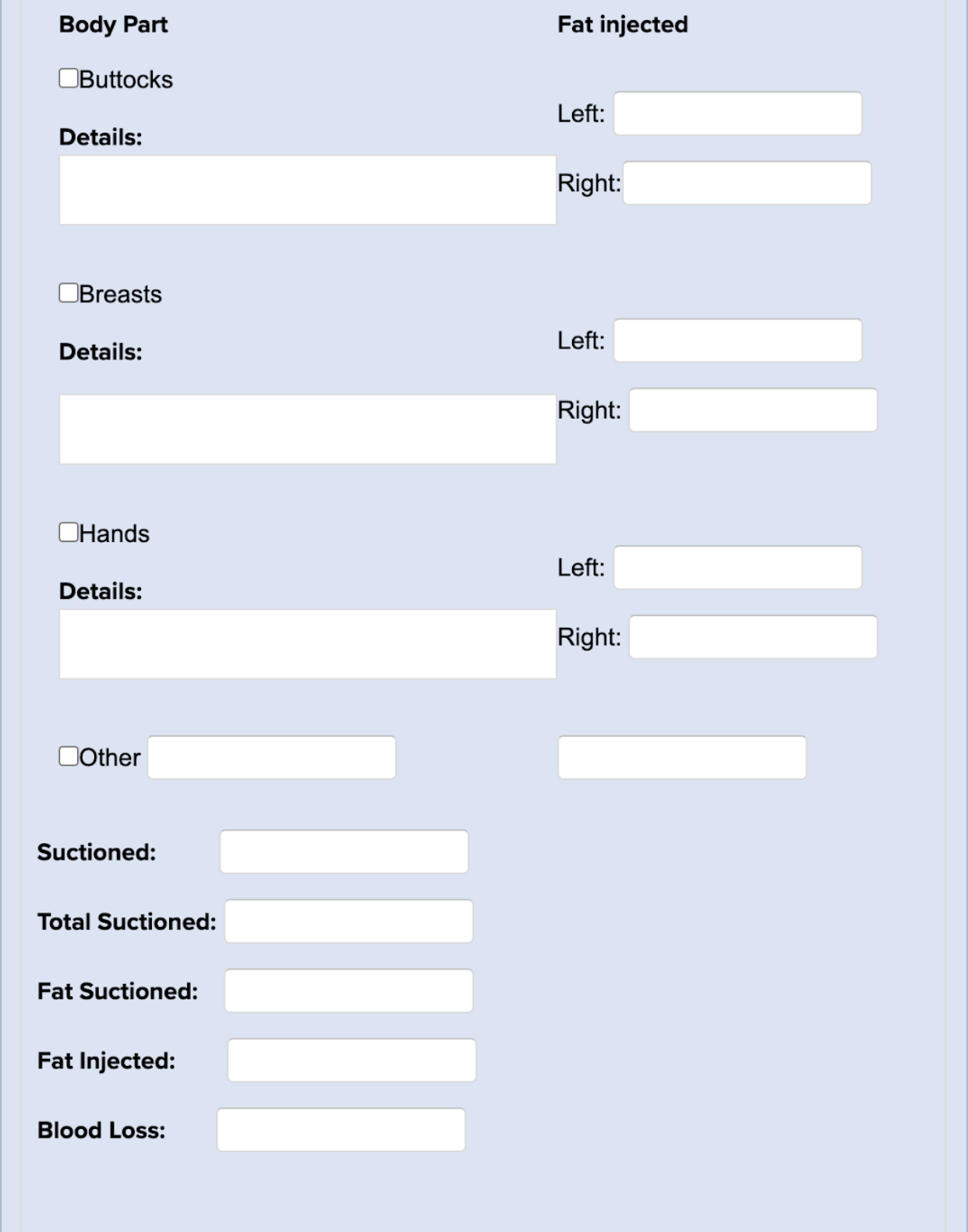
Brazilian Butt Lift - Fat Grafting
Clear & Brilliant Treatment Record
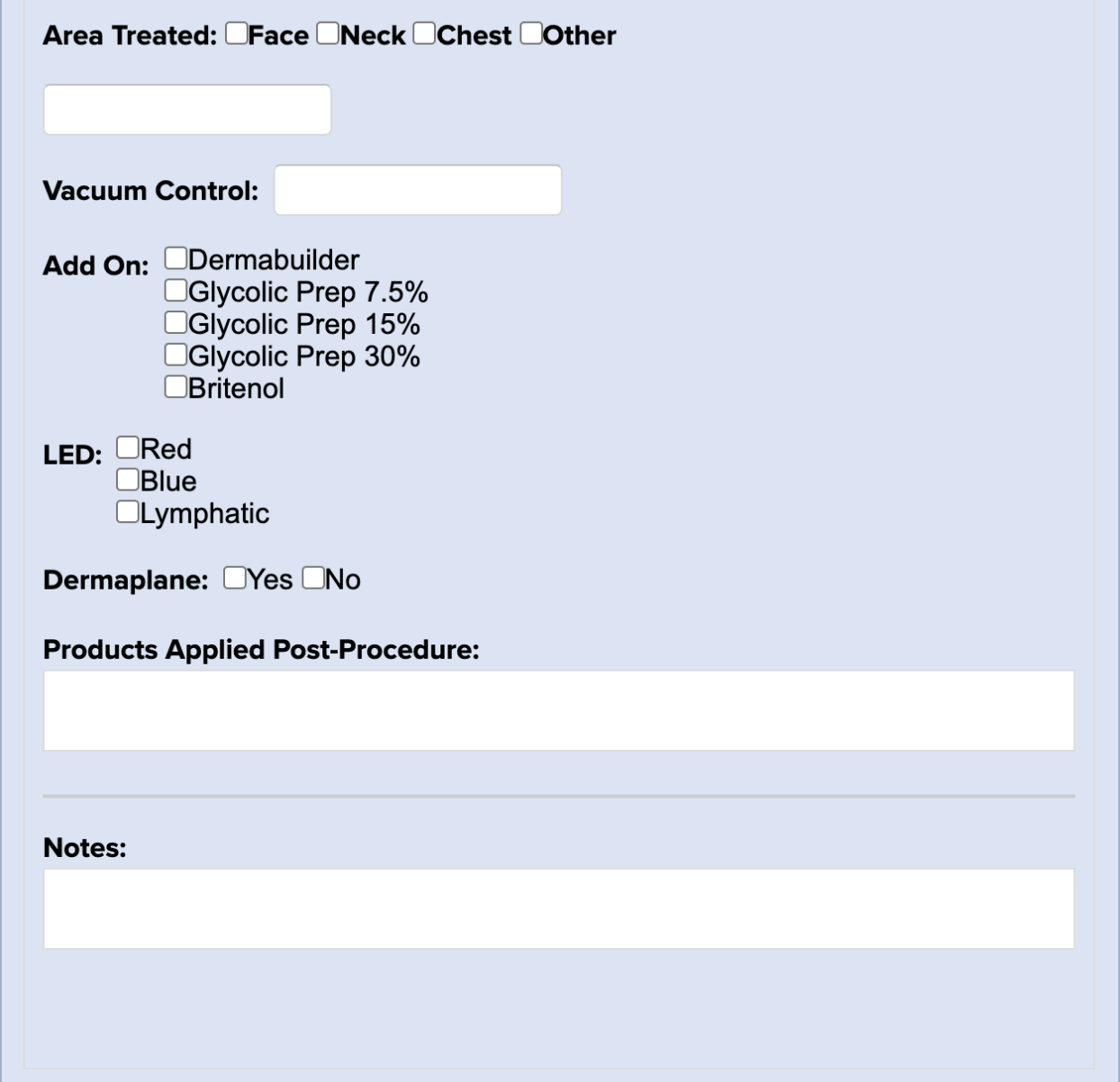
Aesthetician Procedure Note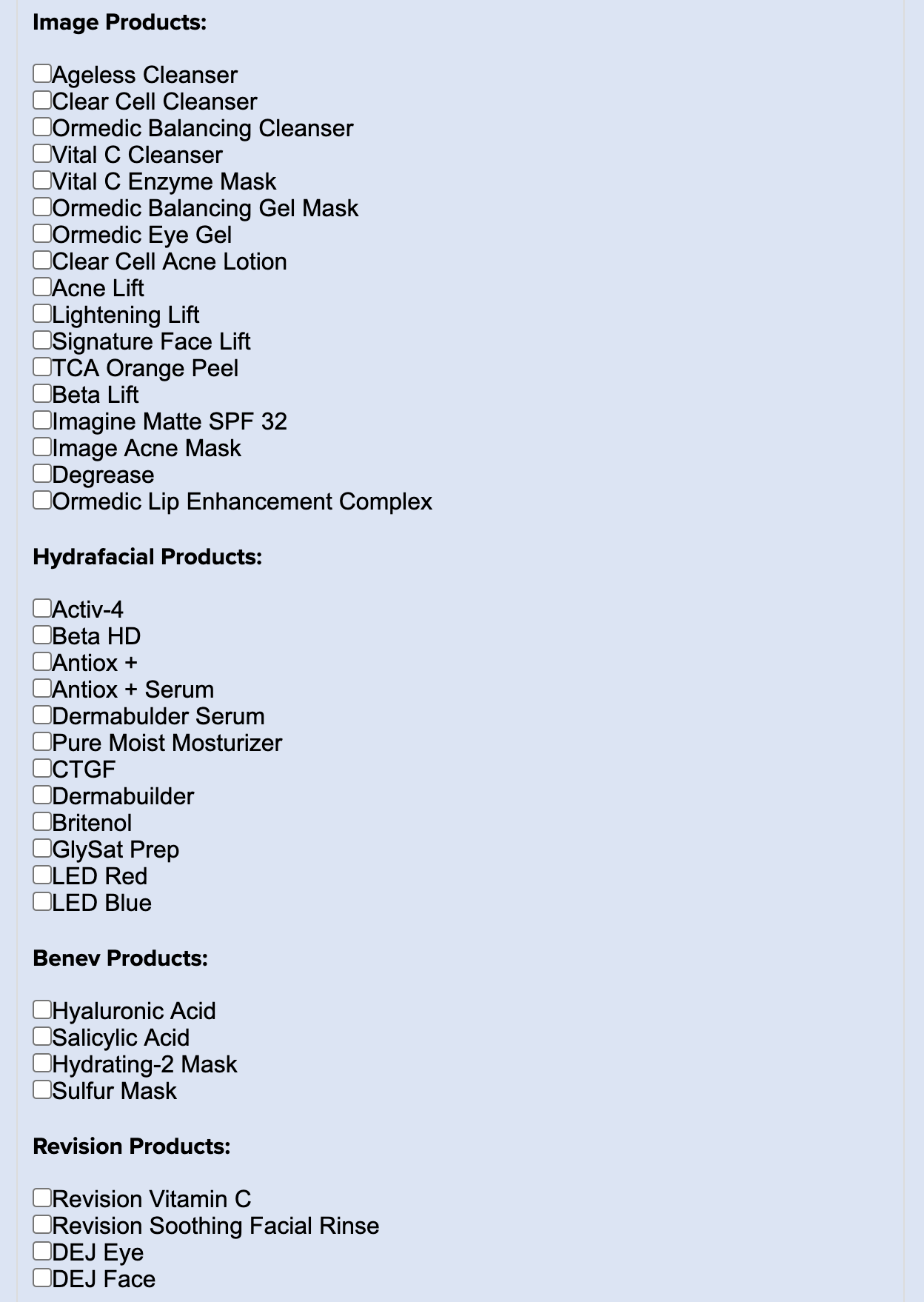
BBL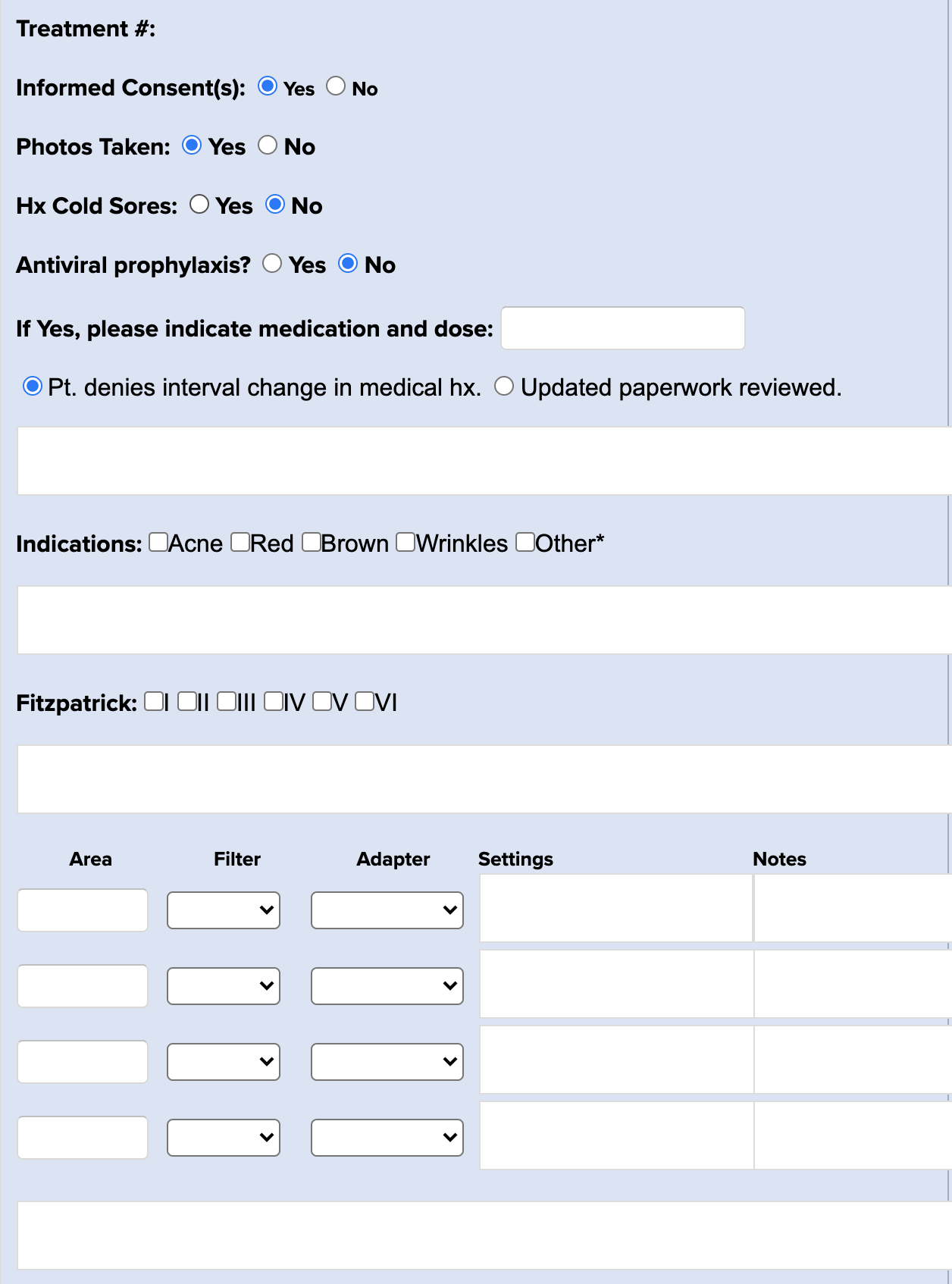
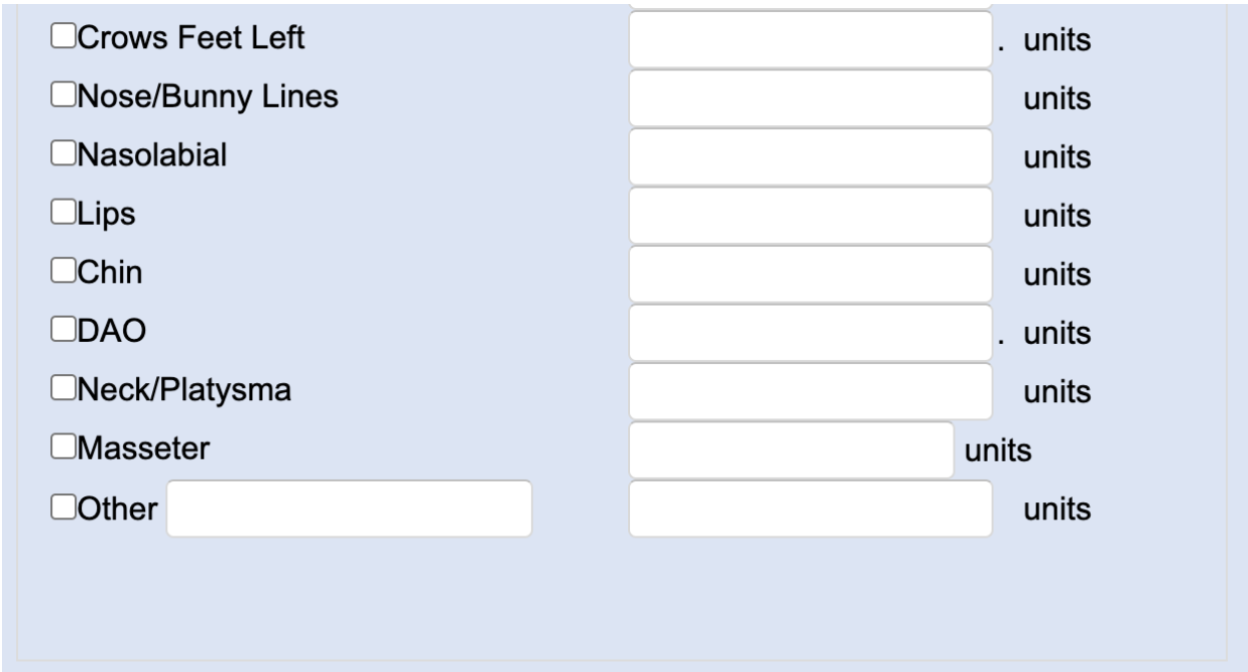
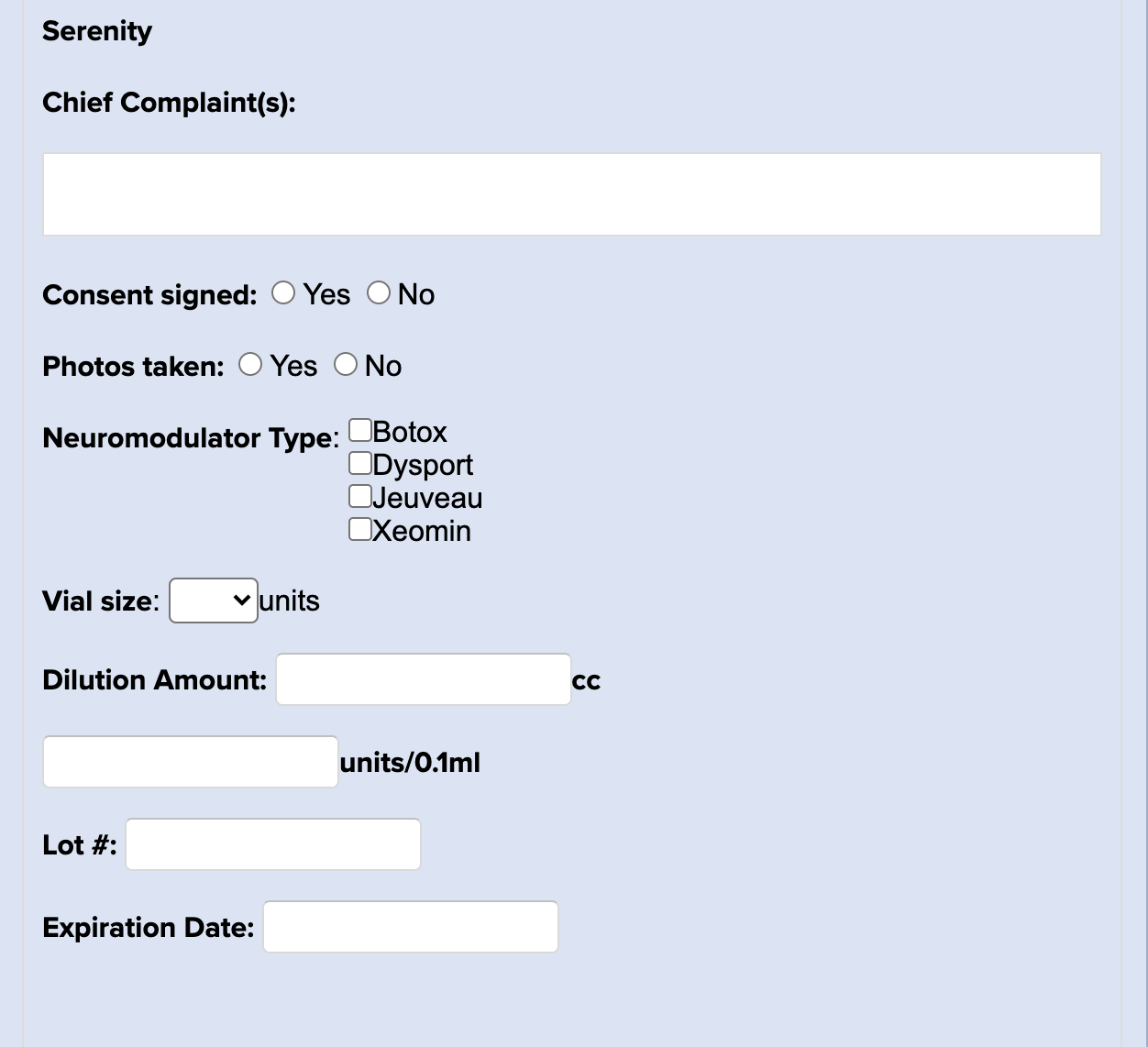
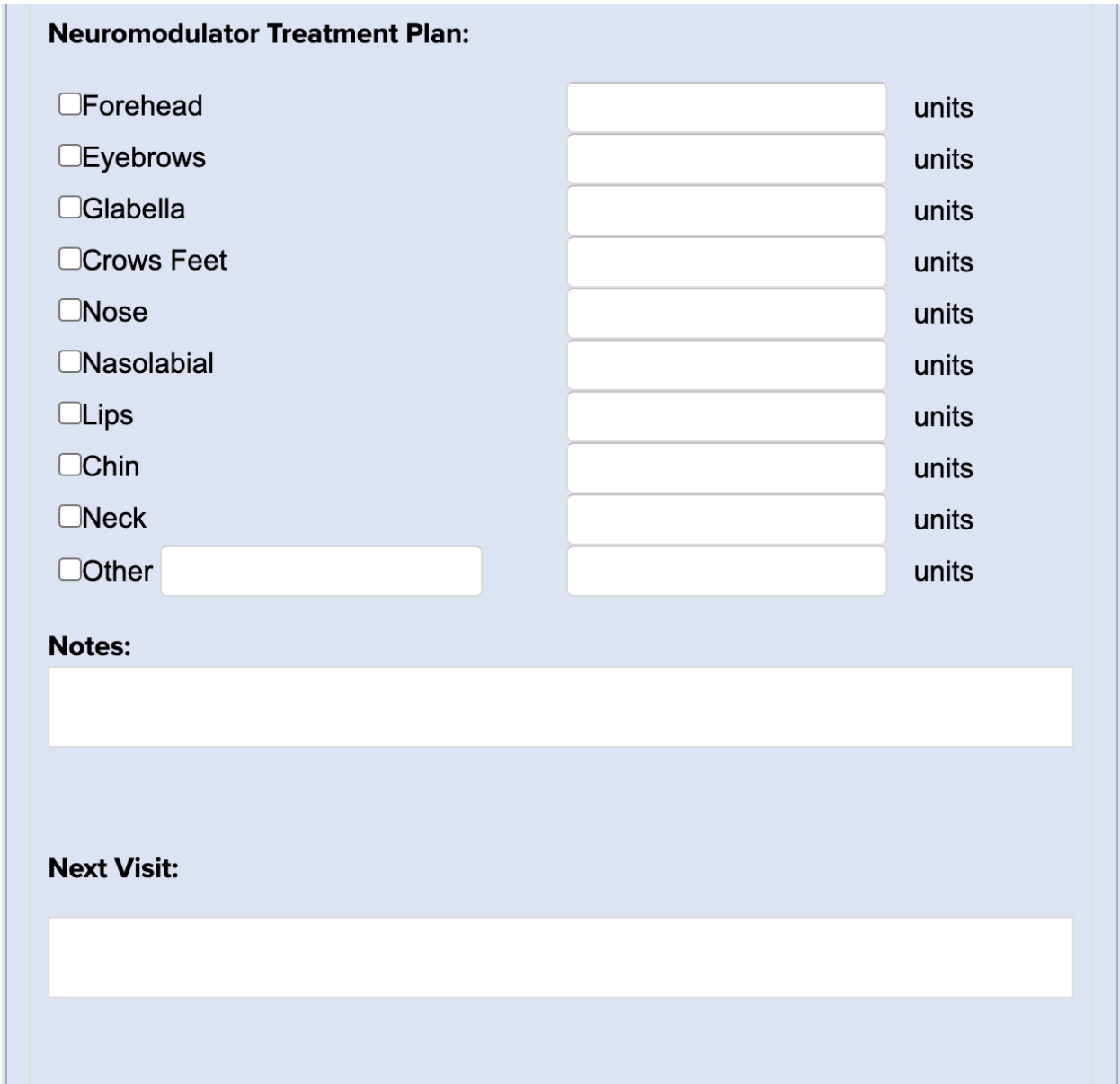
Botox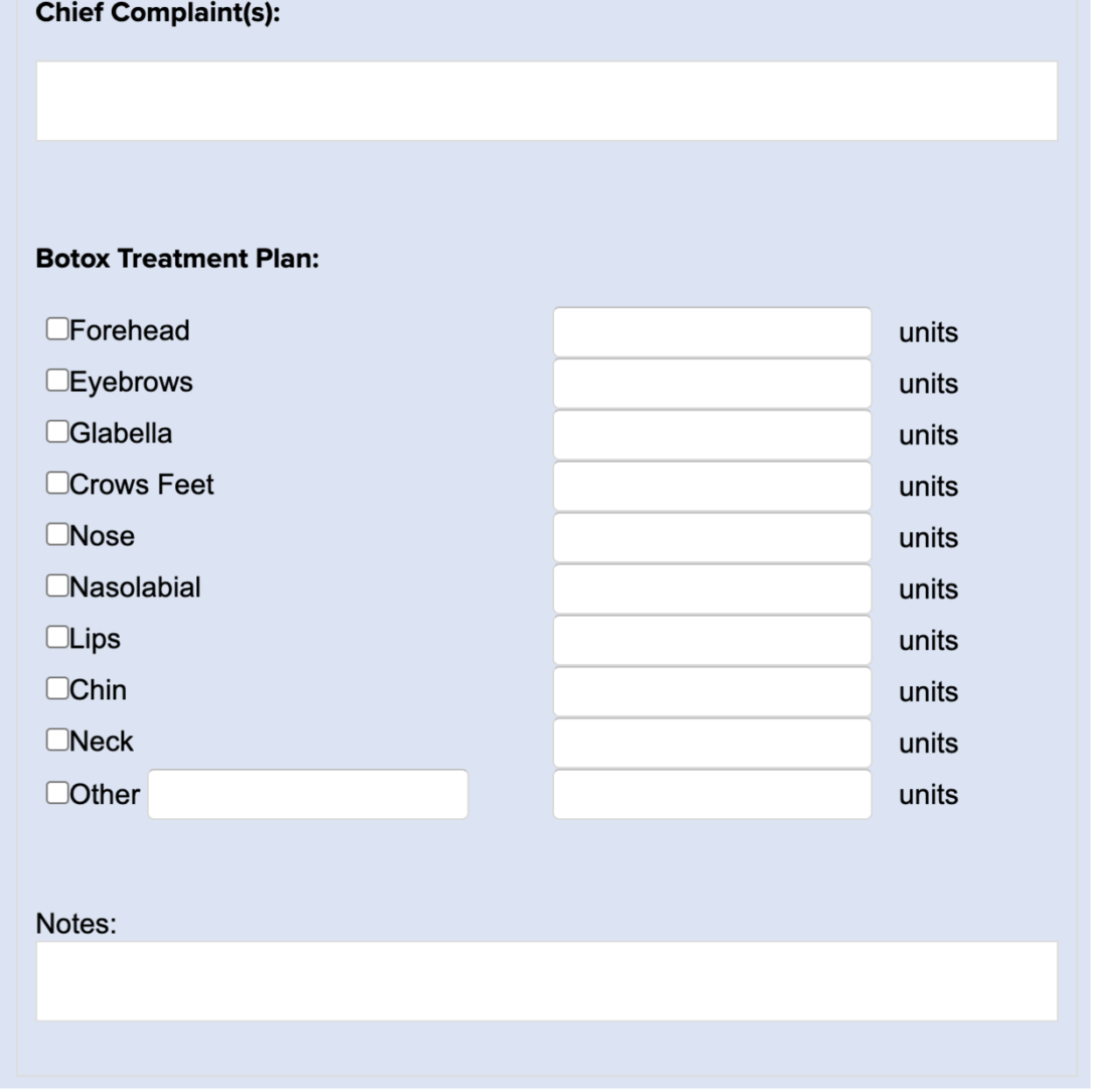
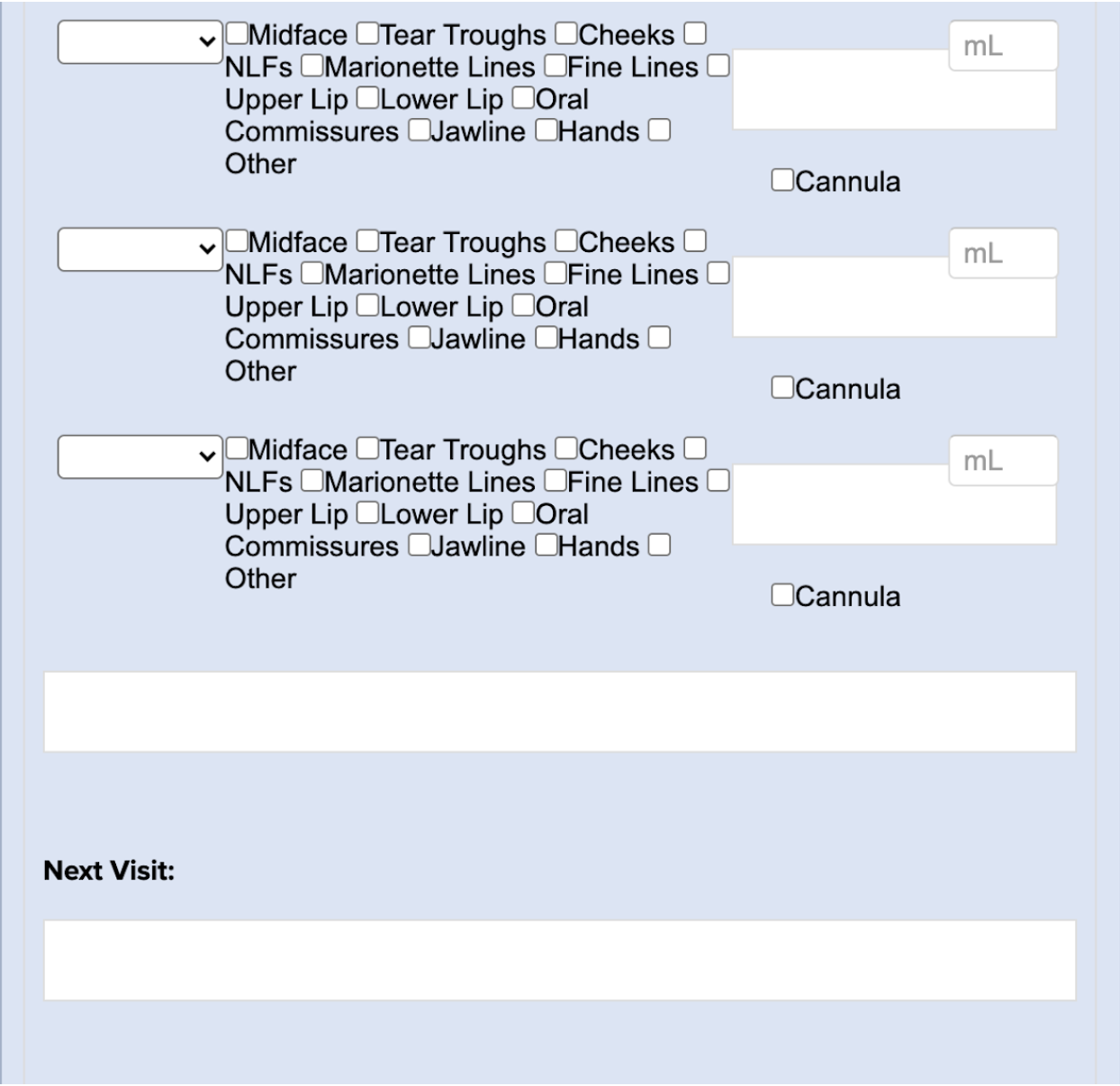
Botox and Filler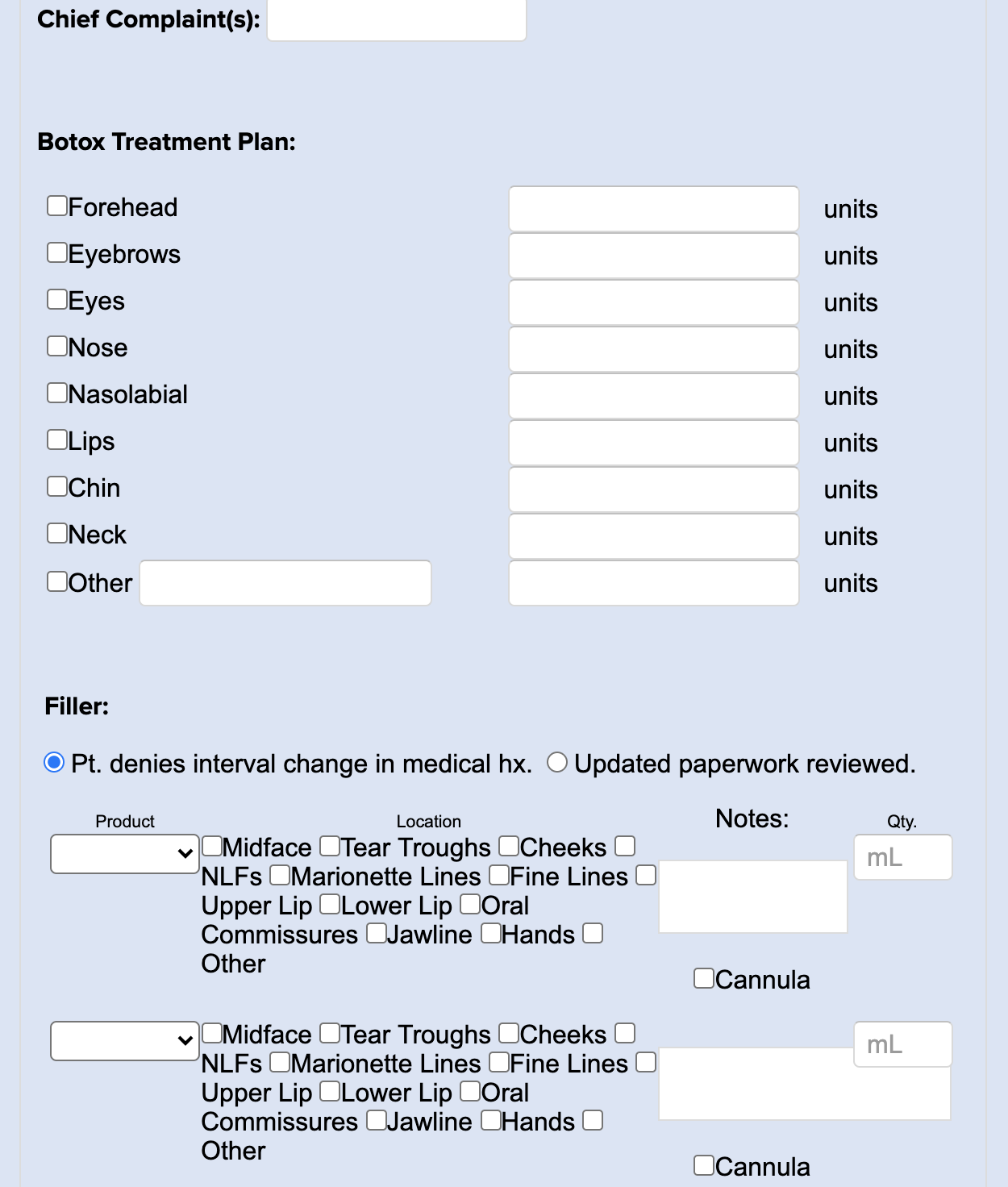
Botox/Dysport/Jeaveau Treatment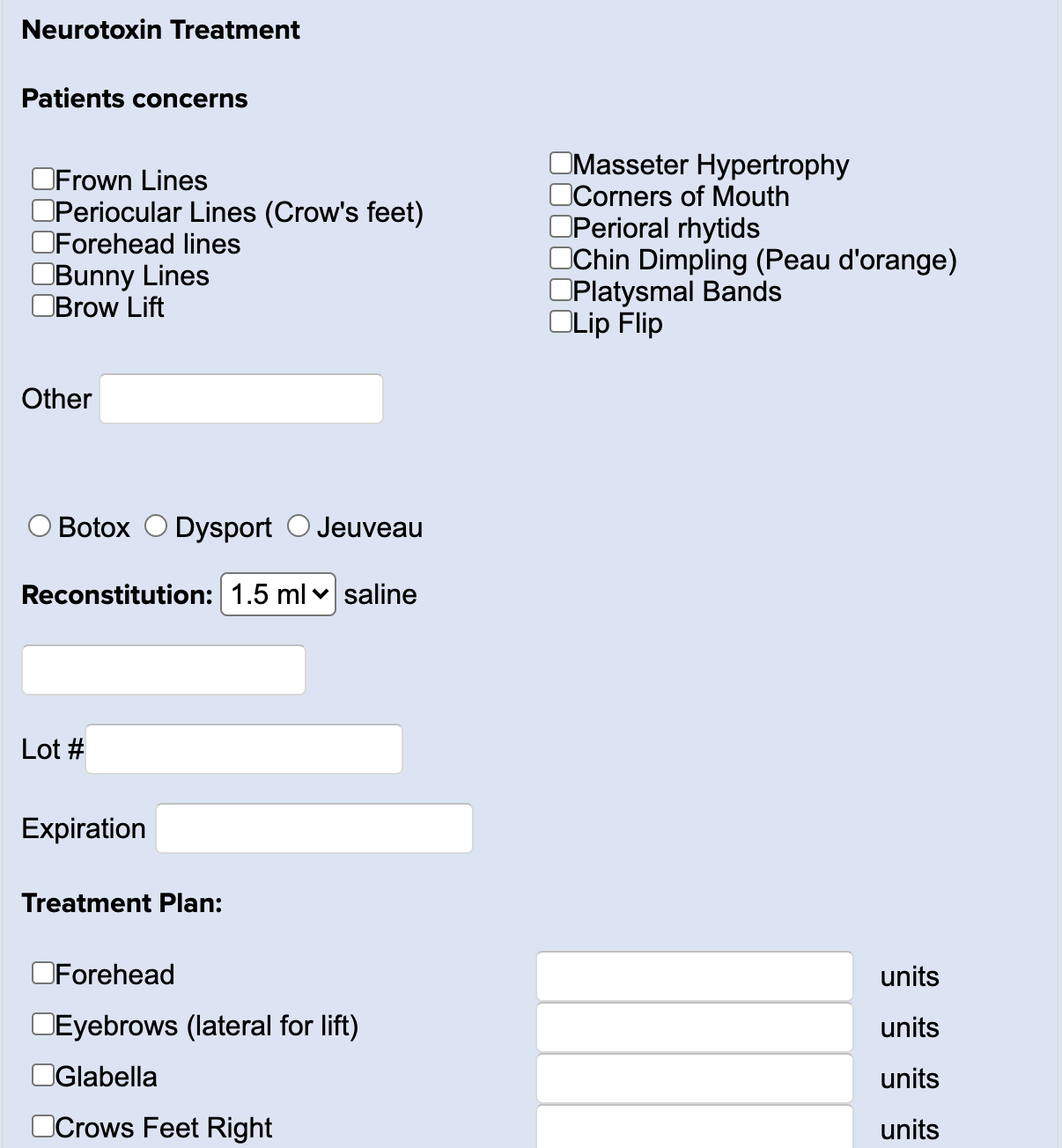
Brachioplasty 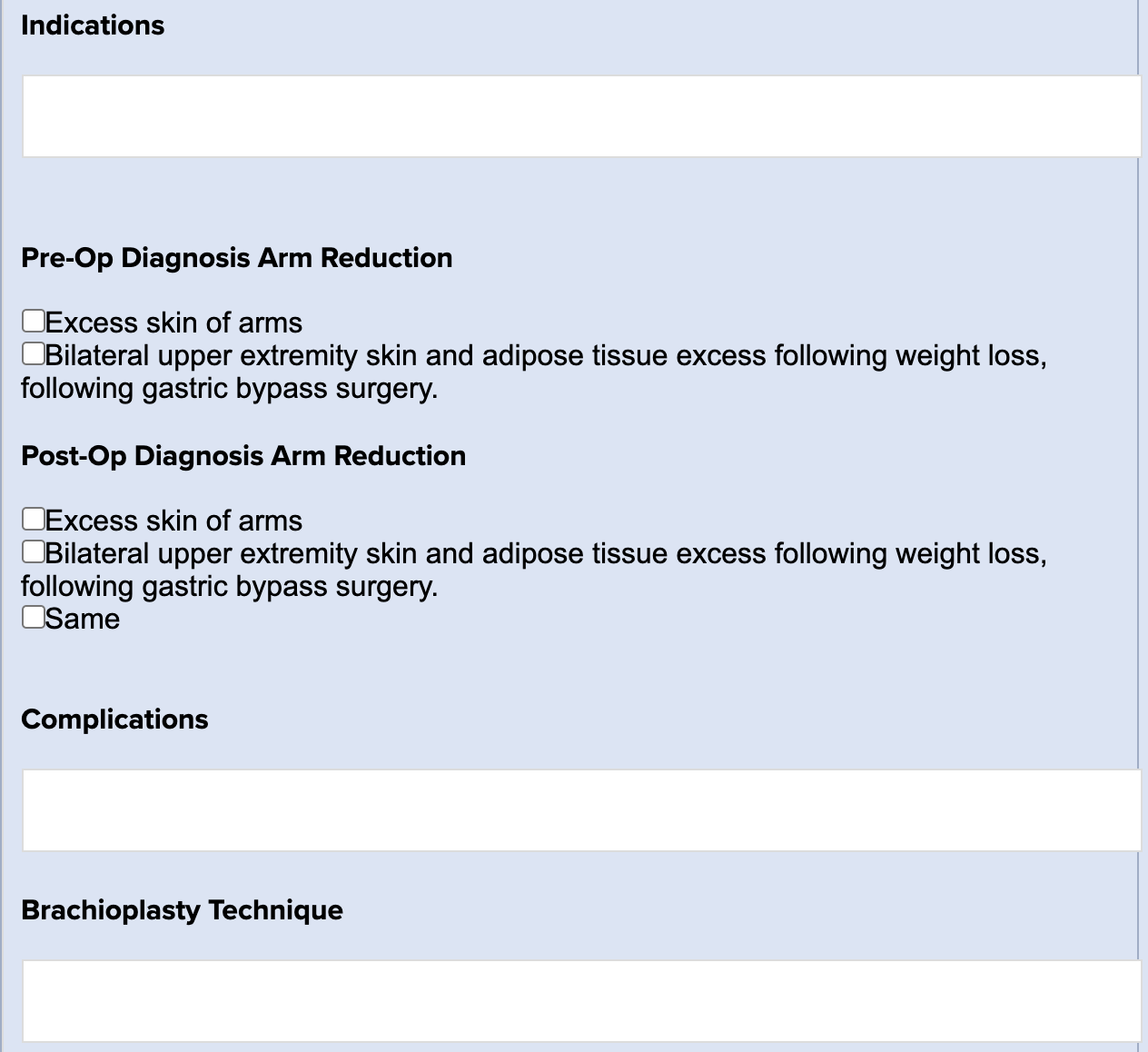
Brachioplasty and Liposuction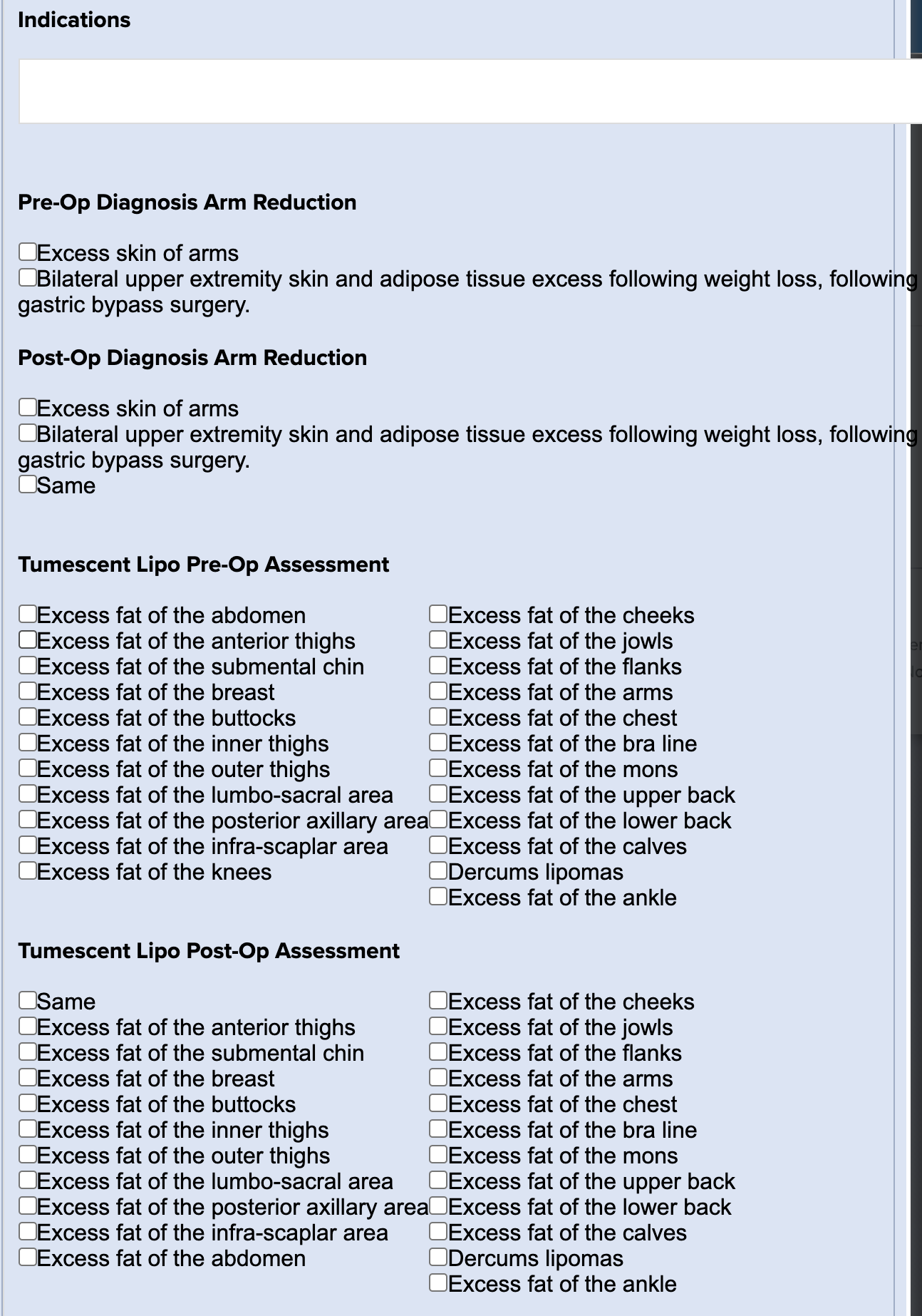
Brazilian Butt Lift - Fat Grafting 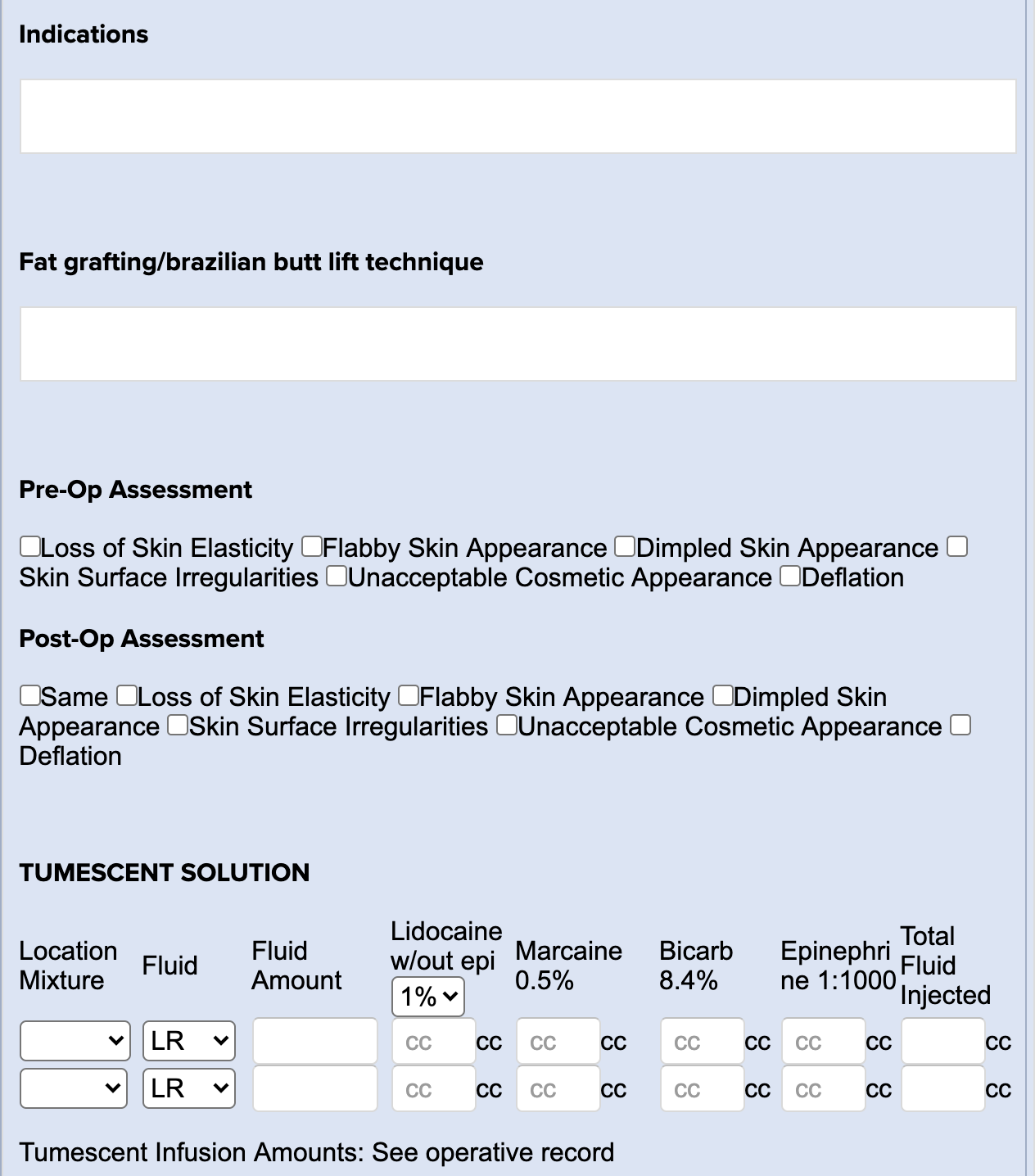
Buccal Fat Removal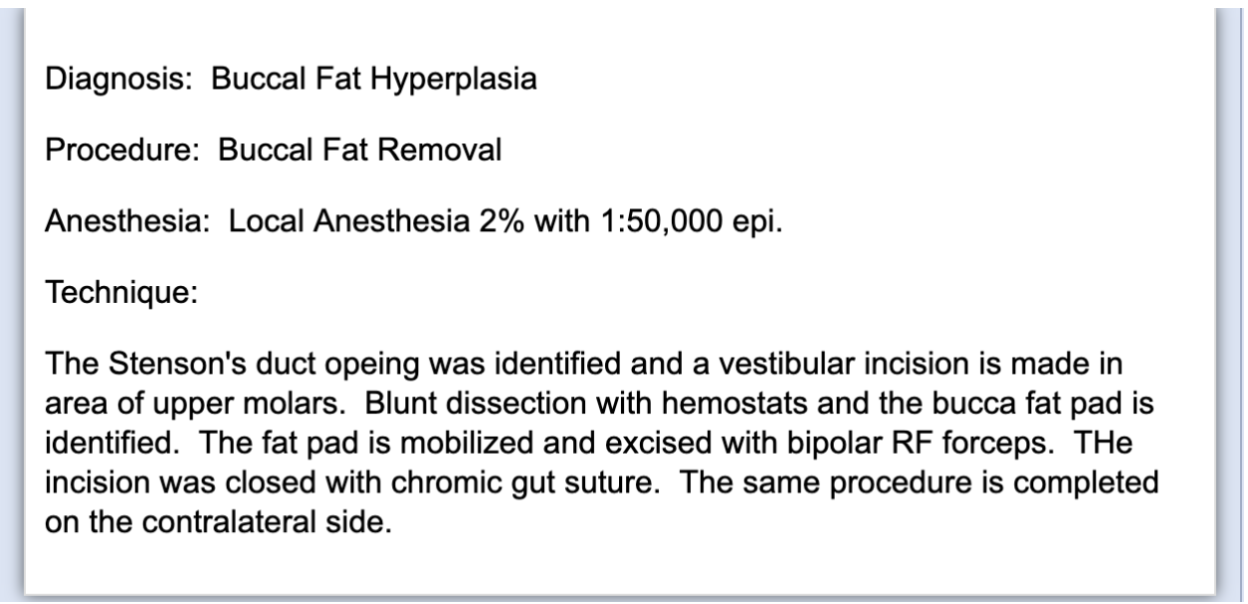
Chemical Peel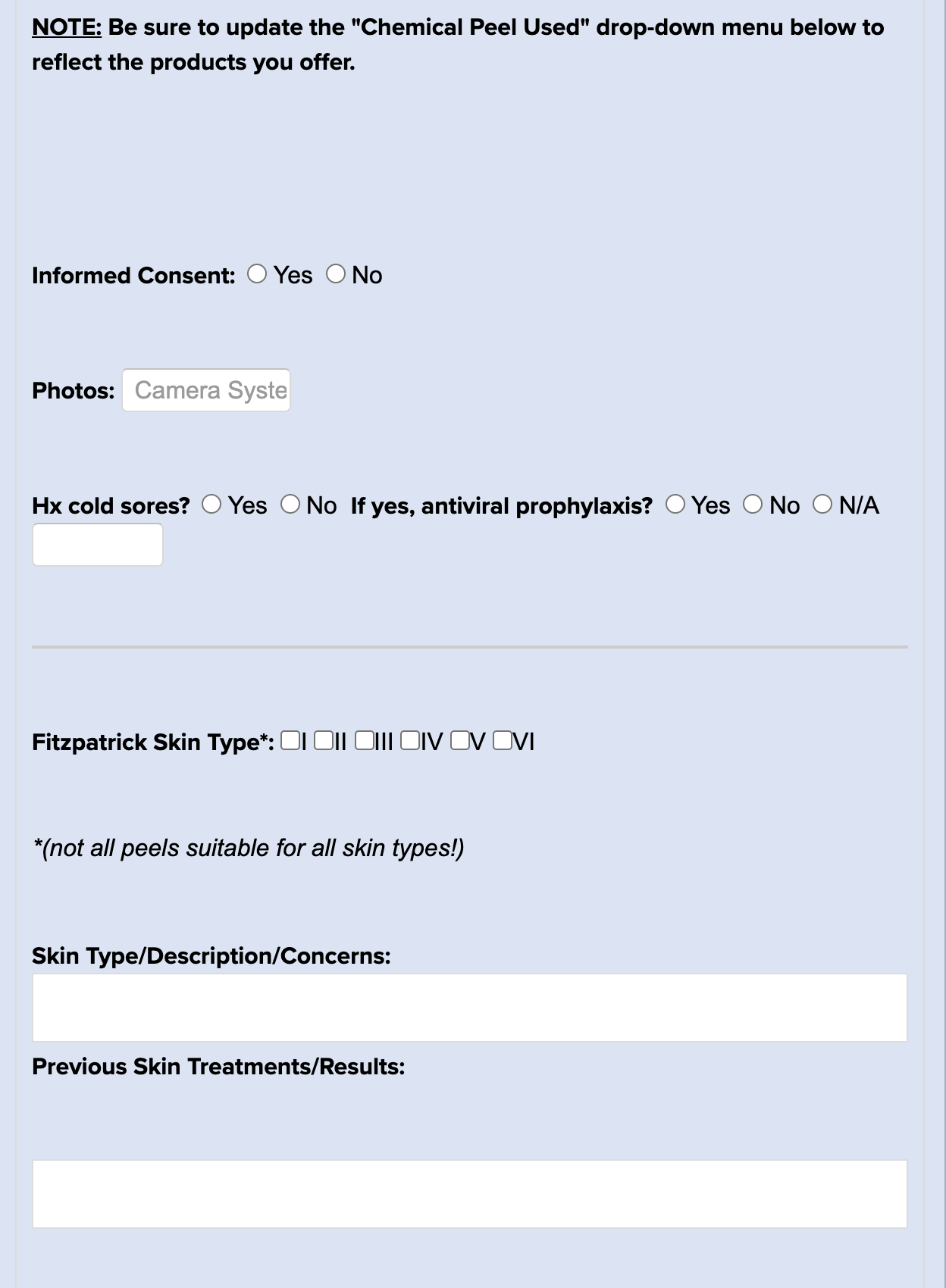
Chiropractic Note
Clear & Brilliant Treatment Record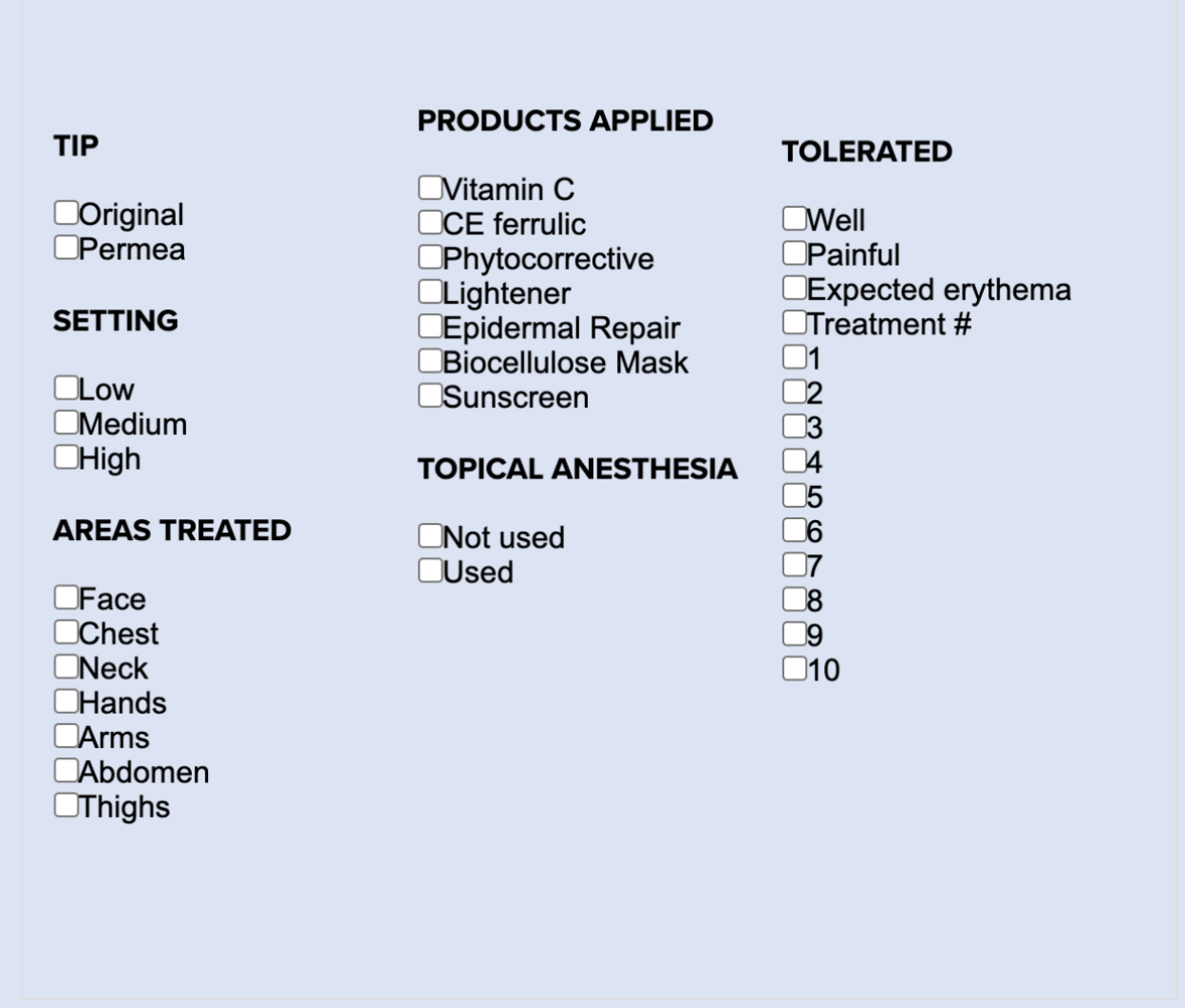
Coolsculpting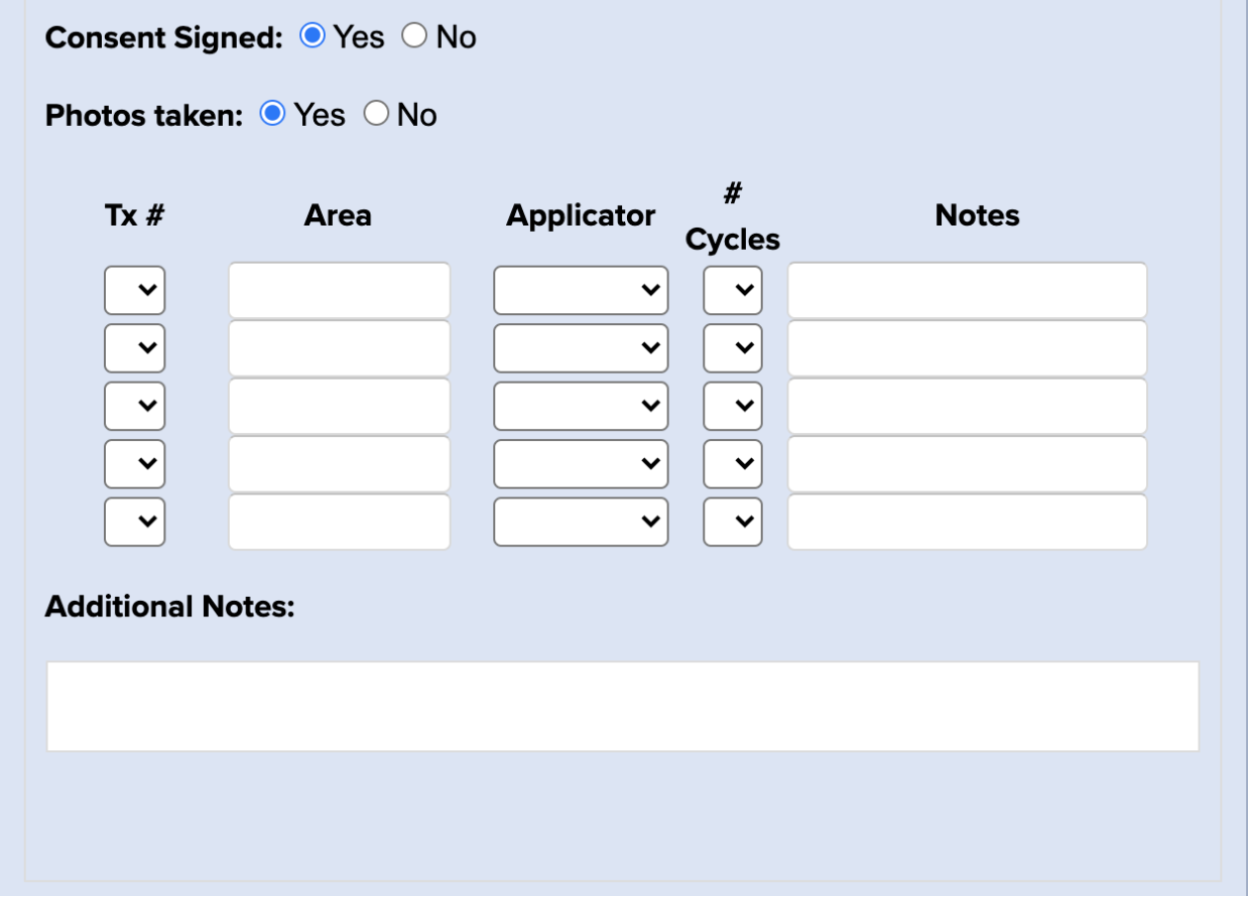
Dermaplane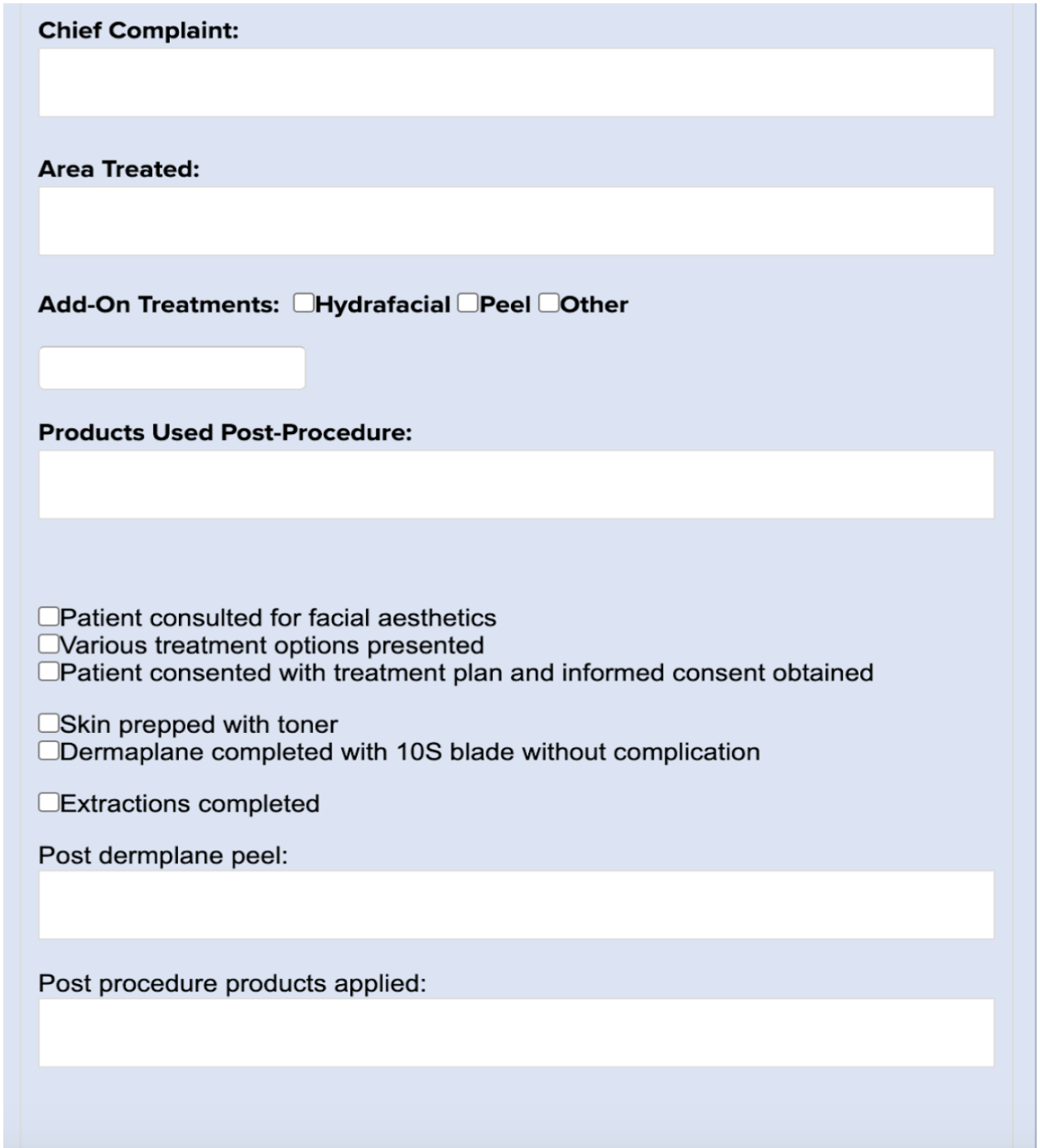
Emsculpt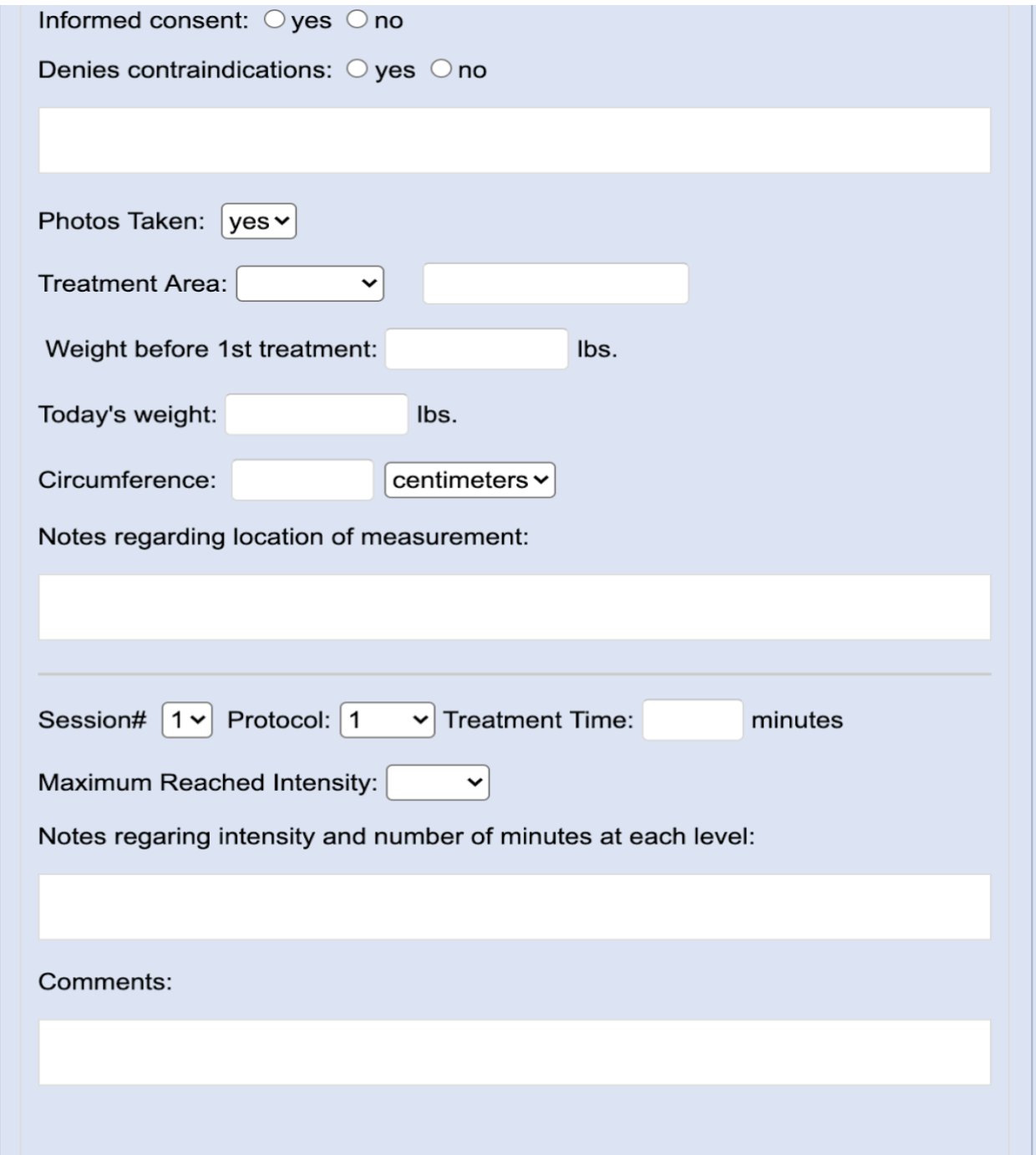
Exilis Ultra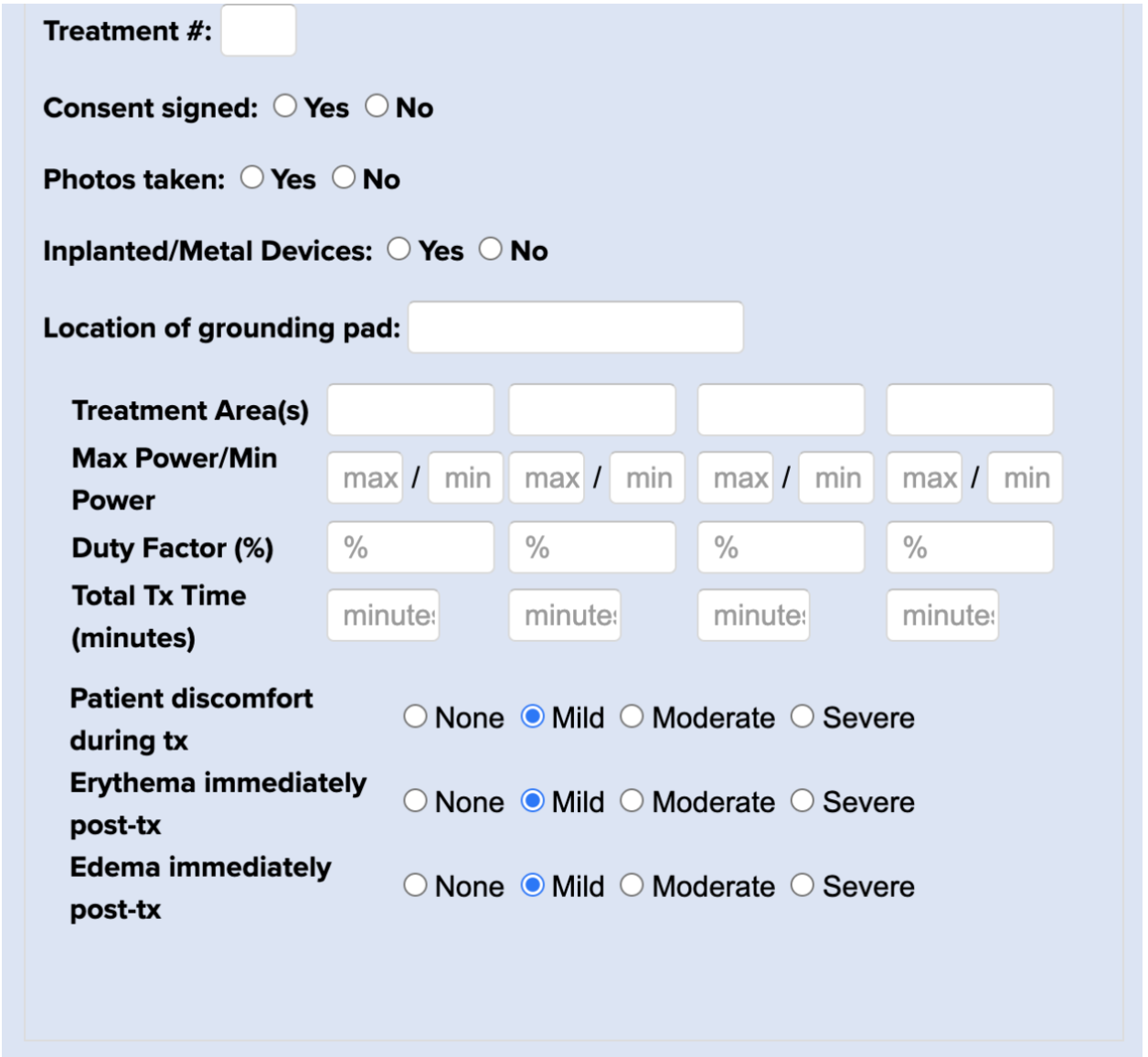
Facelift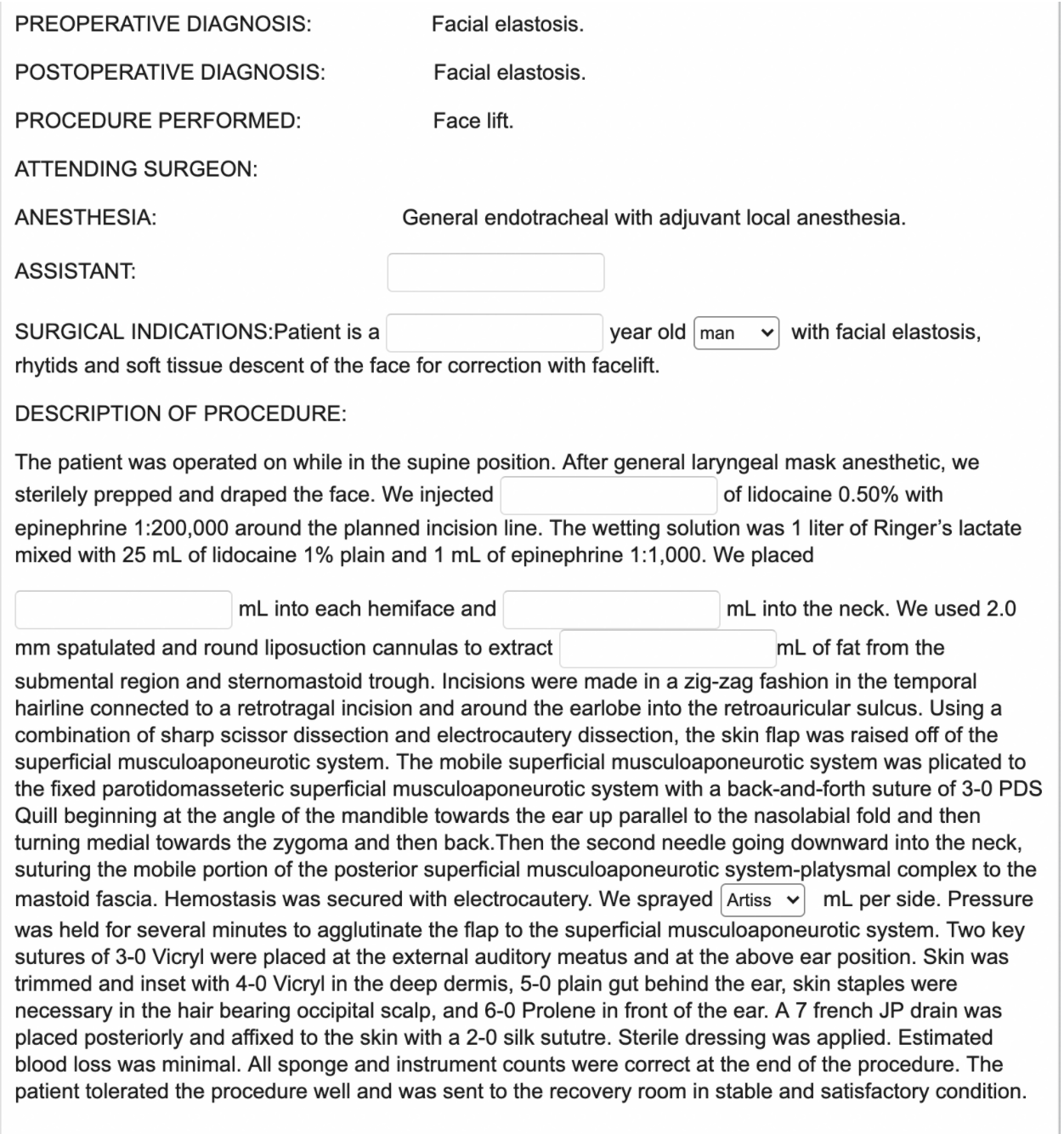
Filter 1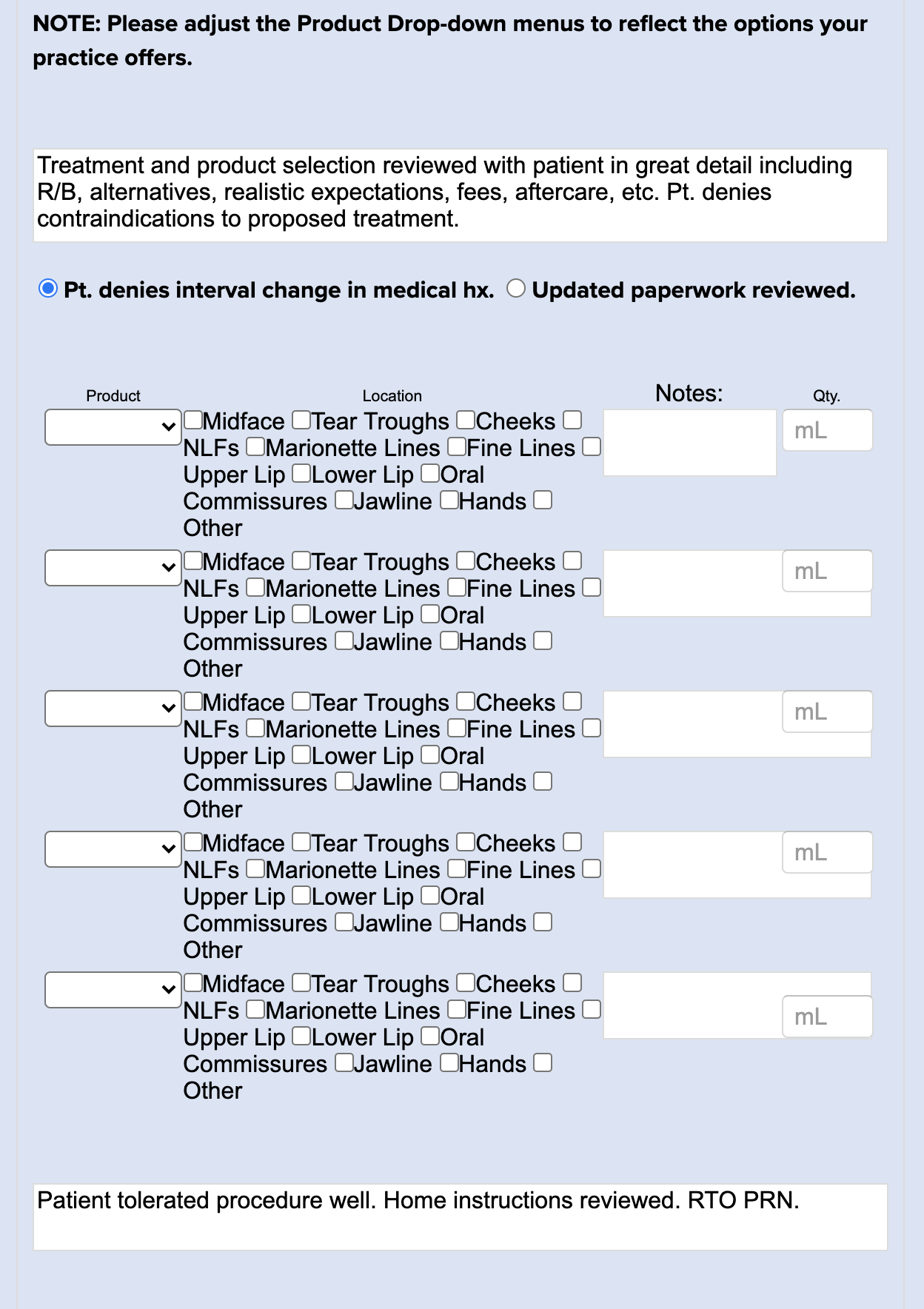
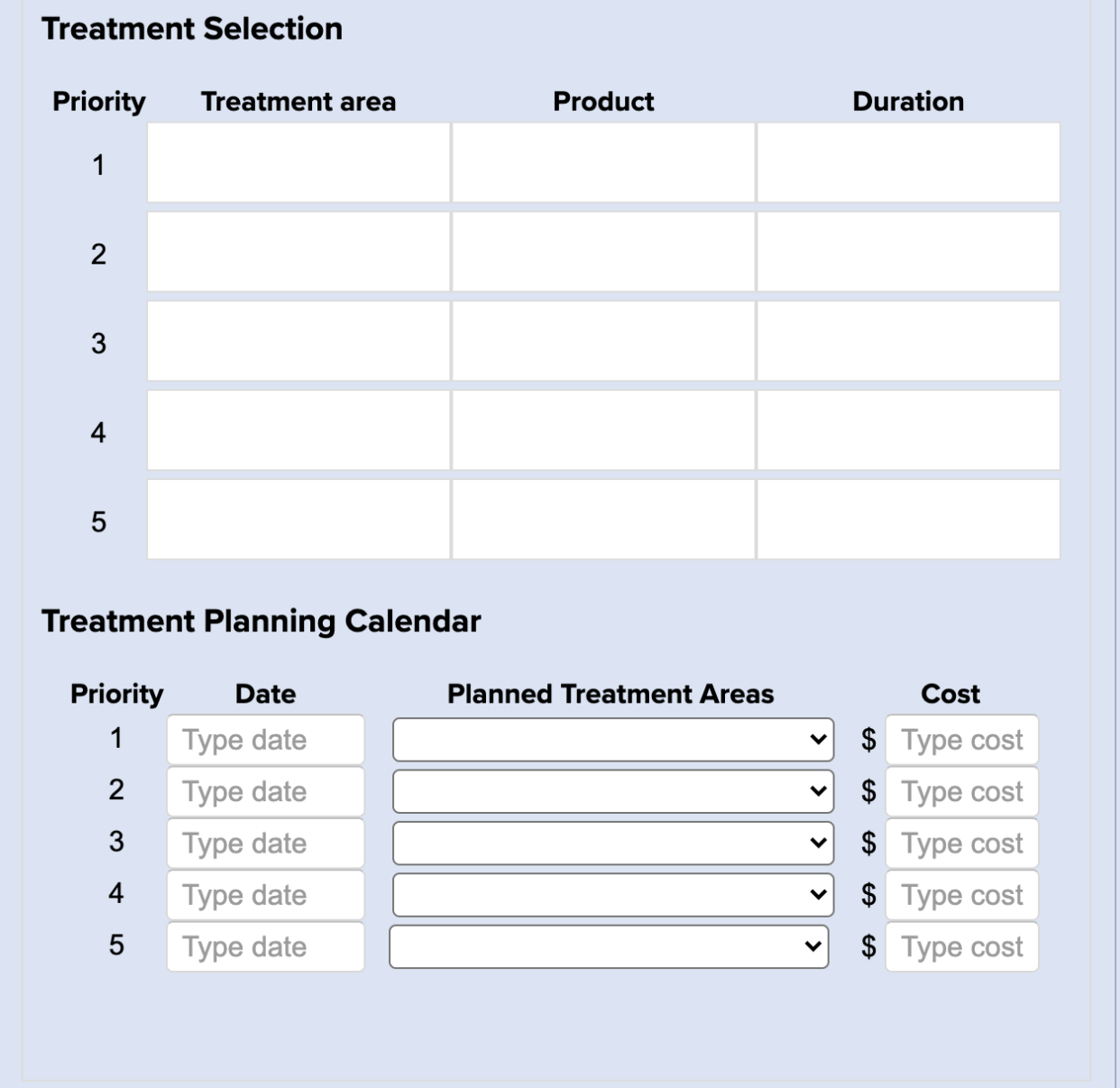
Filter 2 (w/ Care Plan)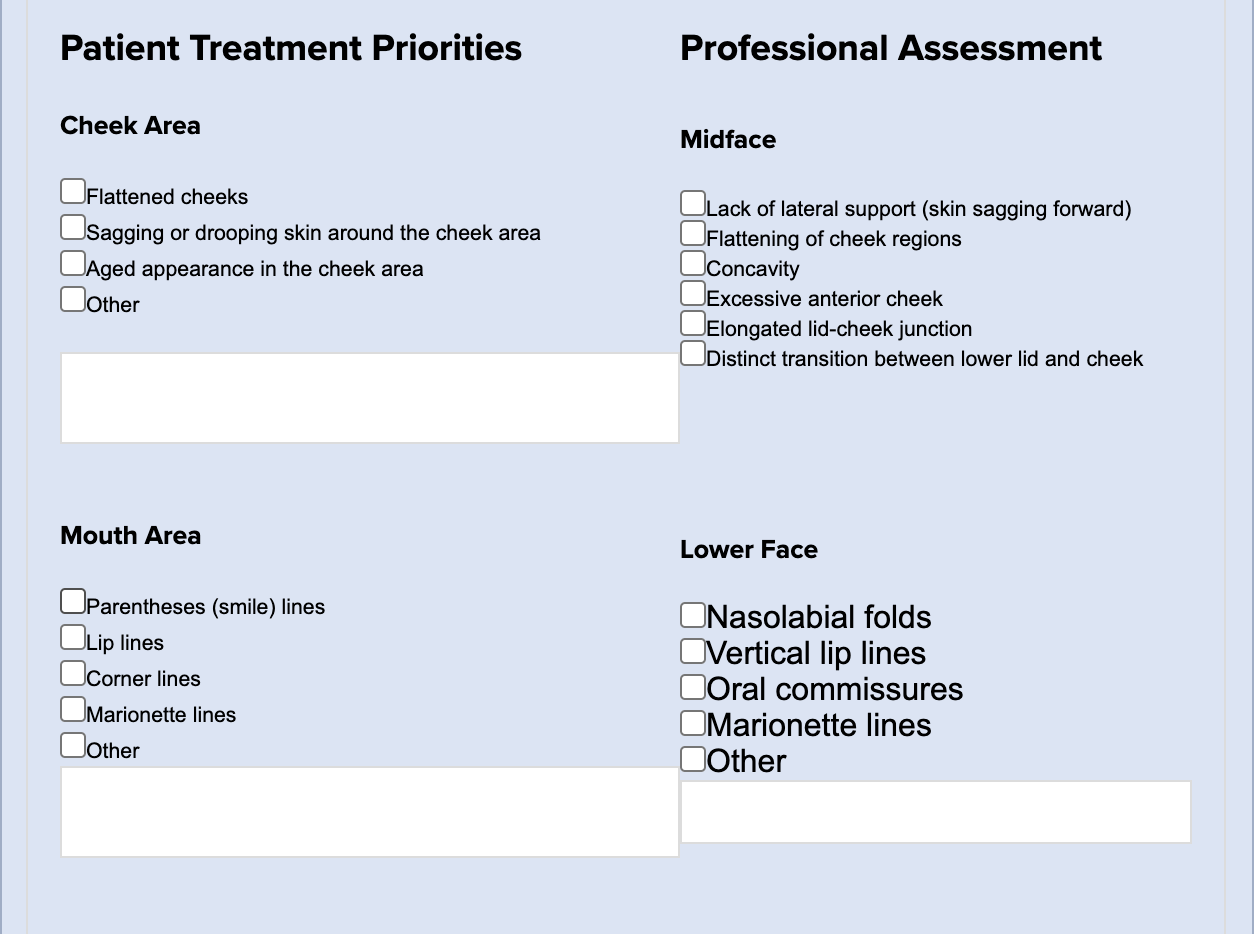
Gynecomastia
Hydrafacial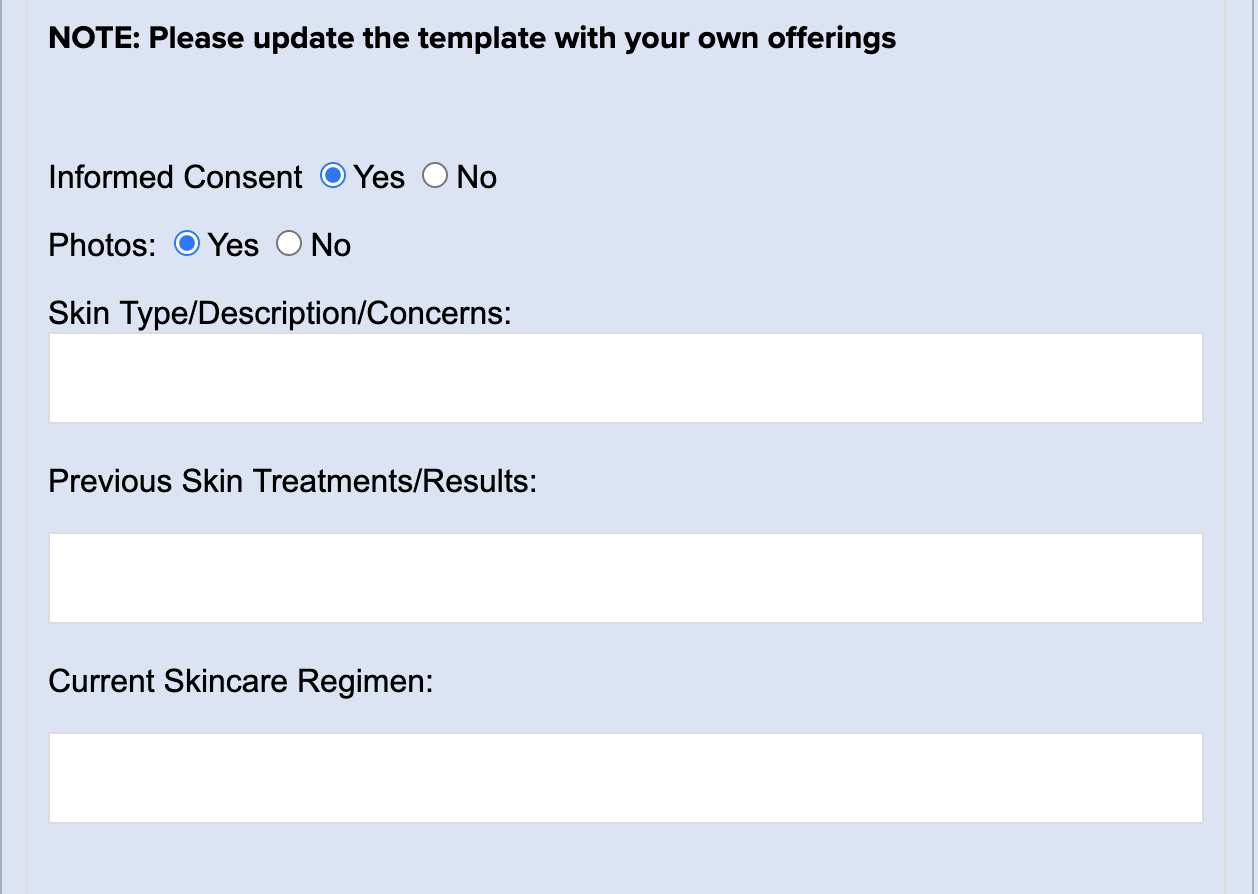
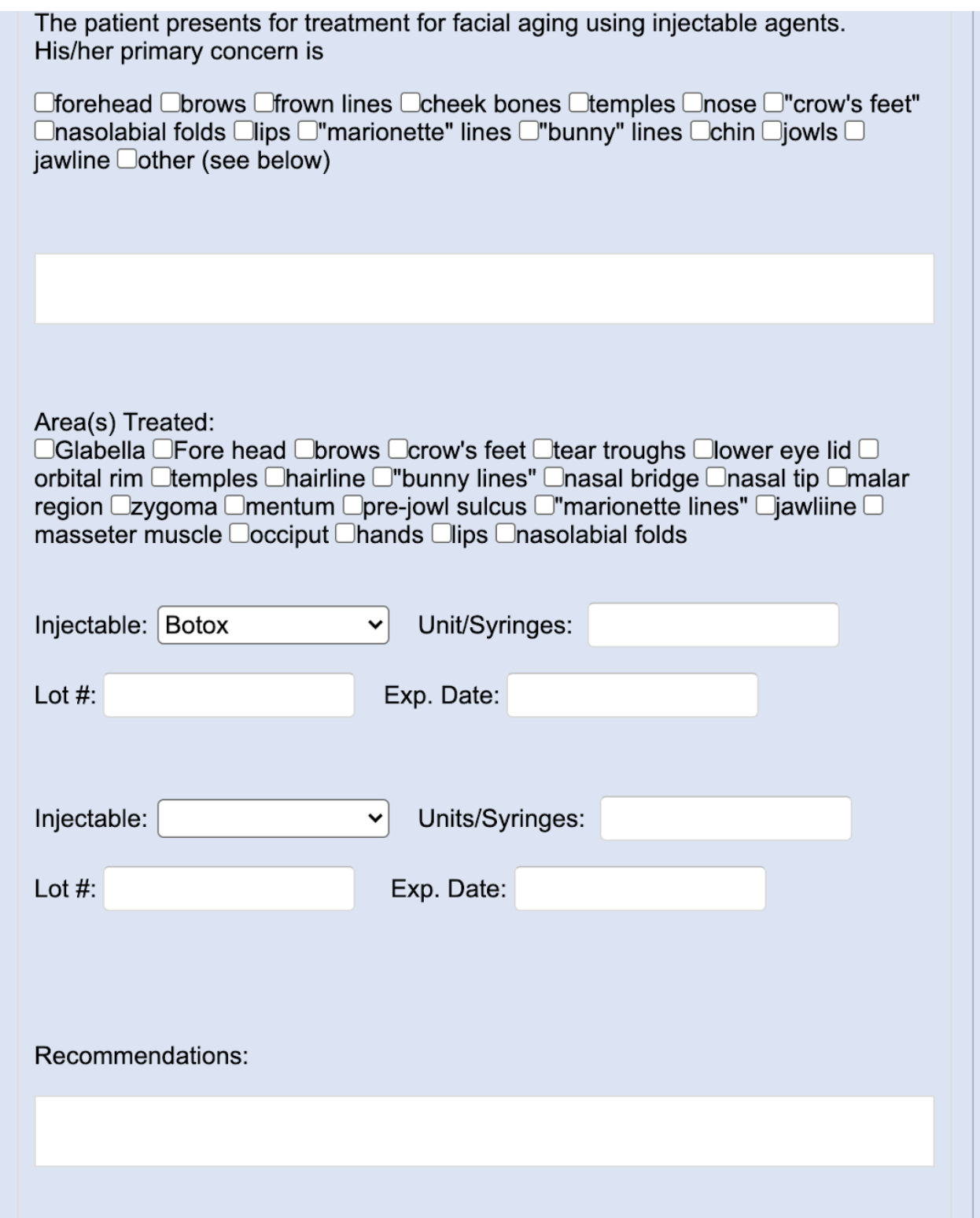
Injectables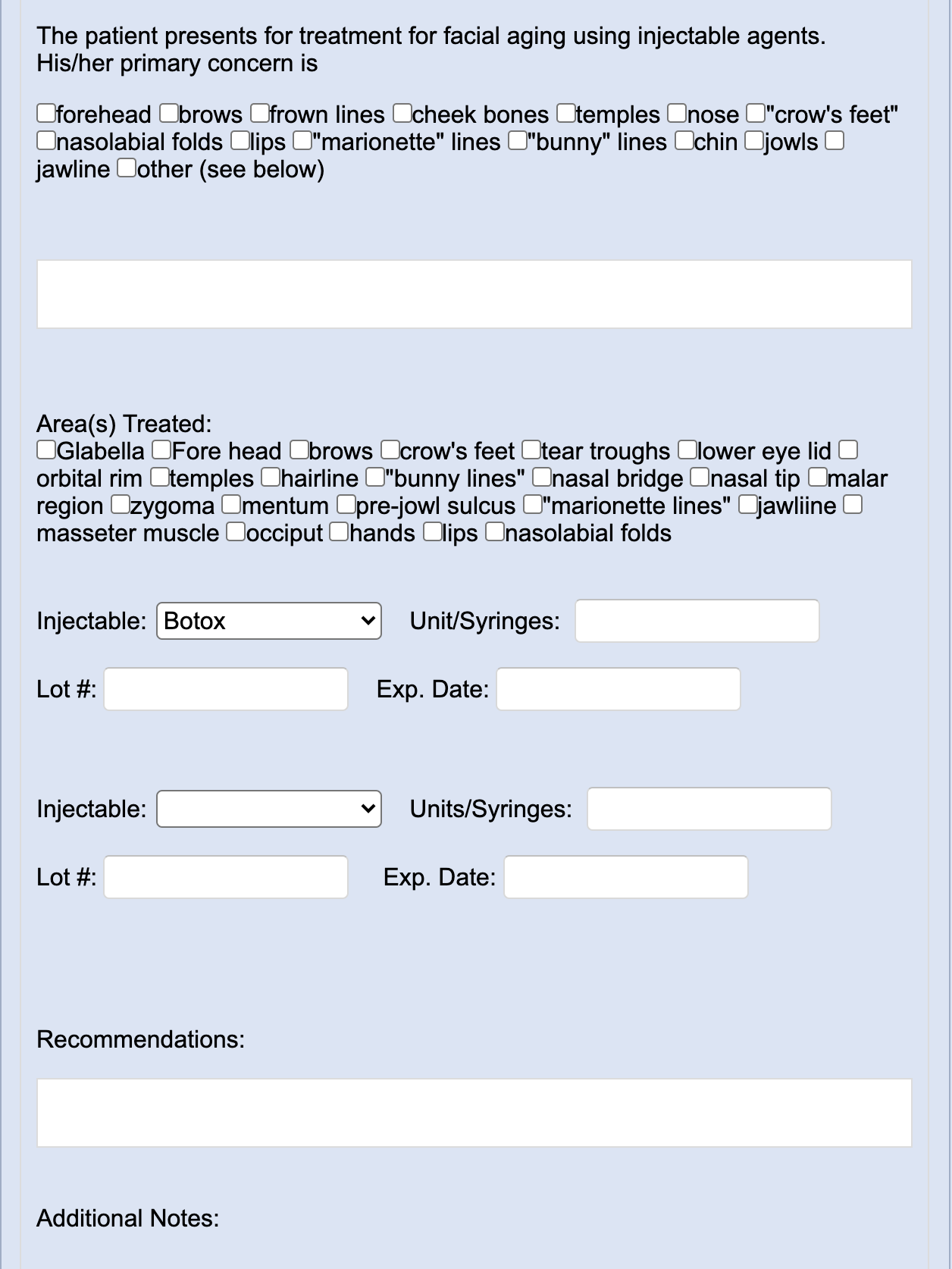
Injection Form - IVs
IV Form
Juvederm (filler)
Kybella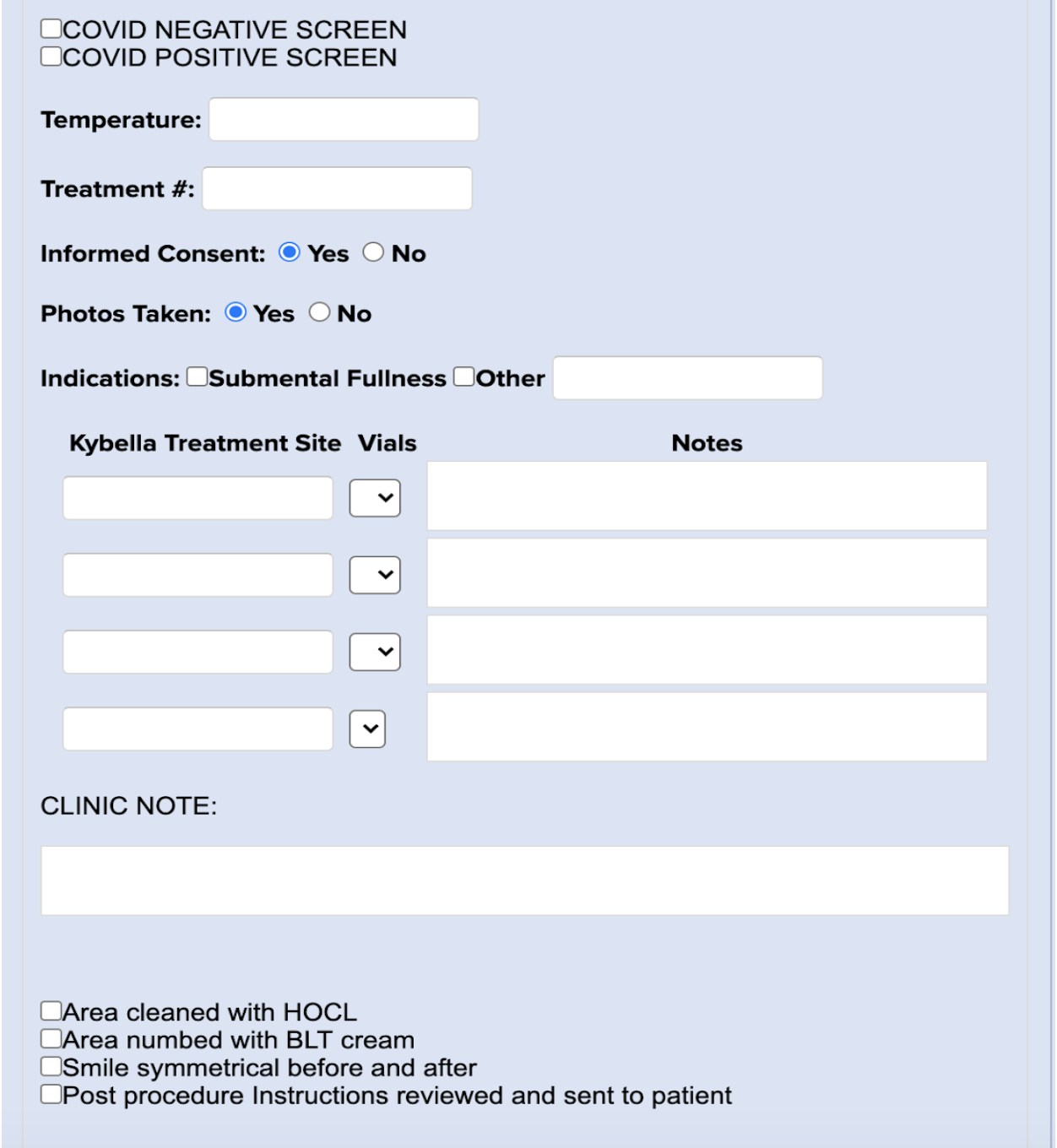
Labiaplastry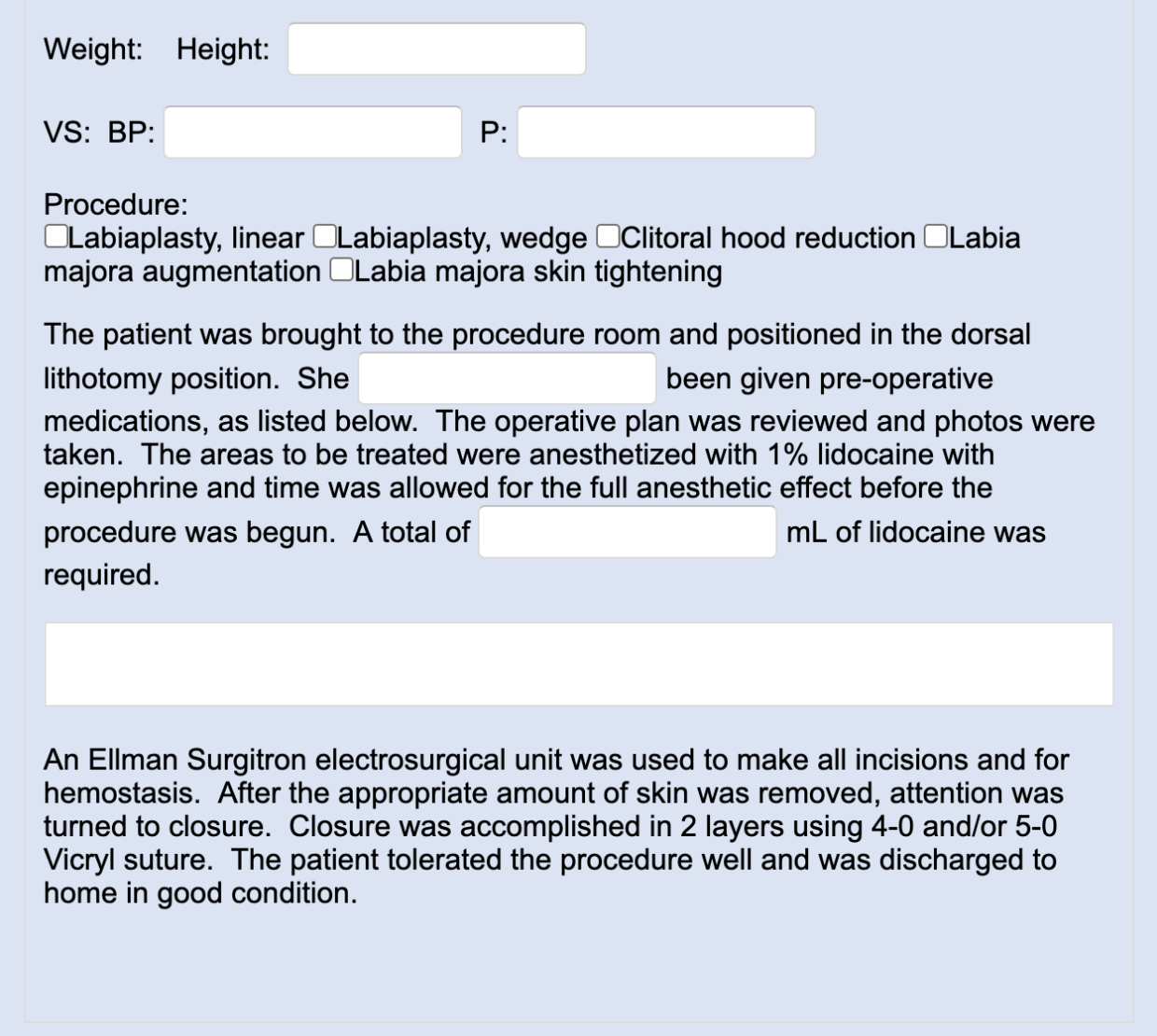
Laser Hair Removal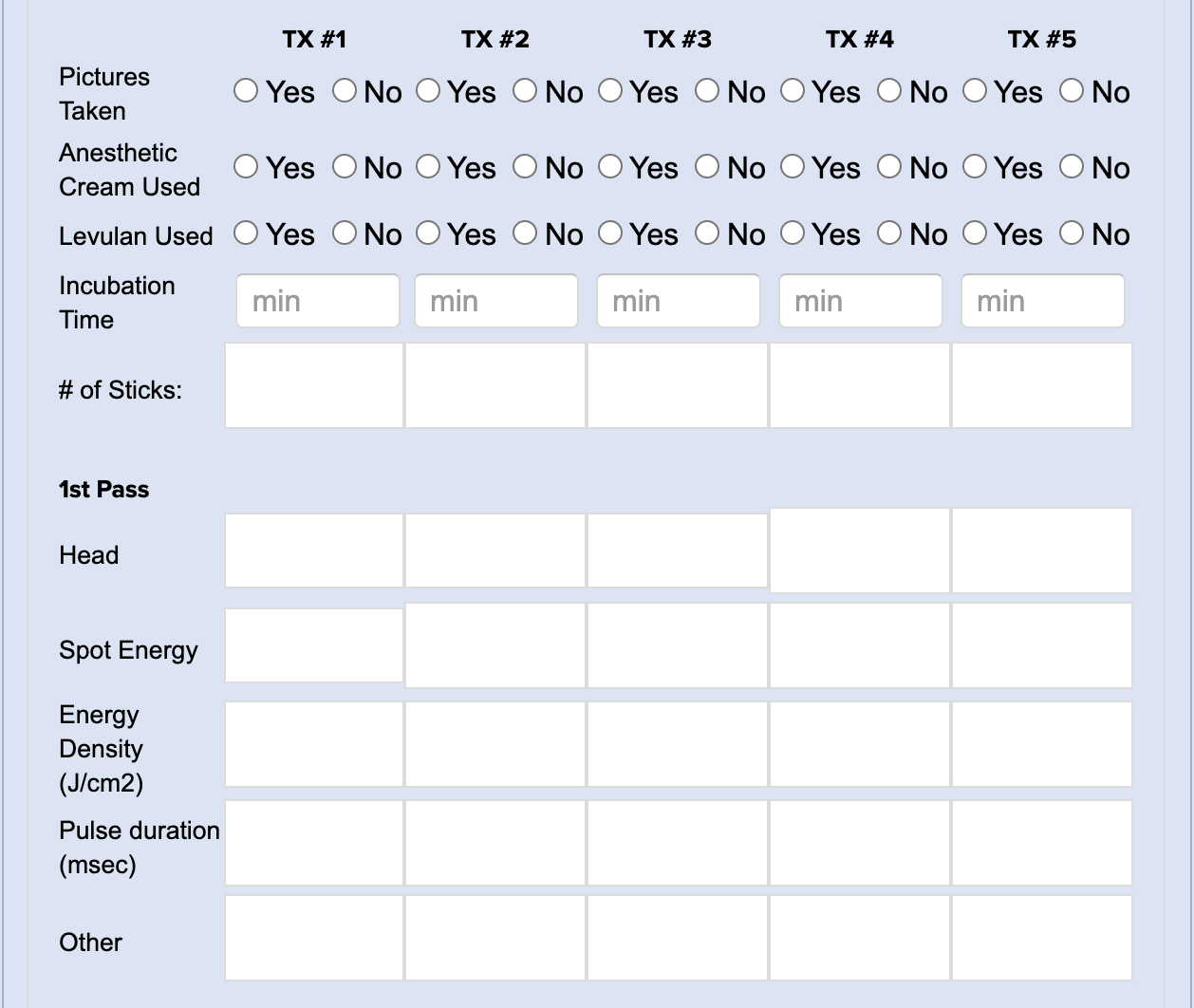
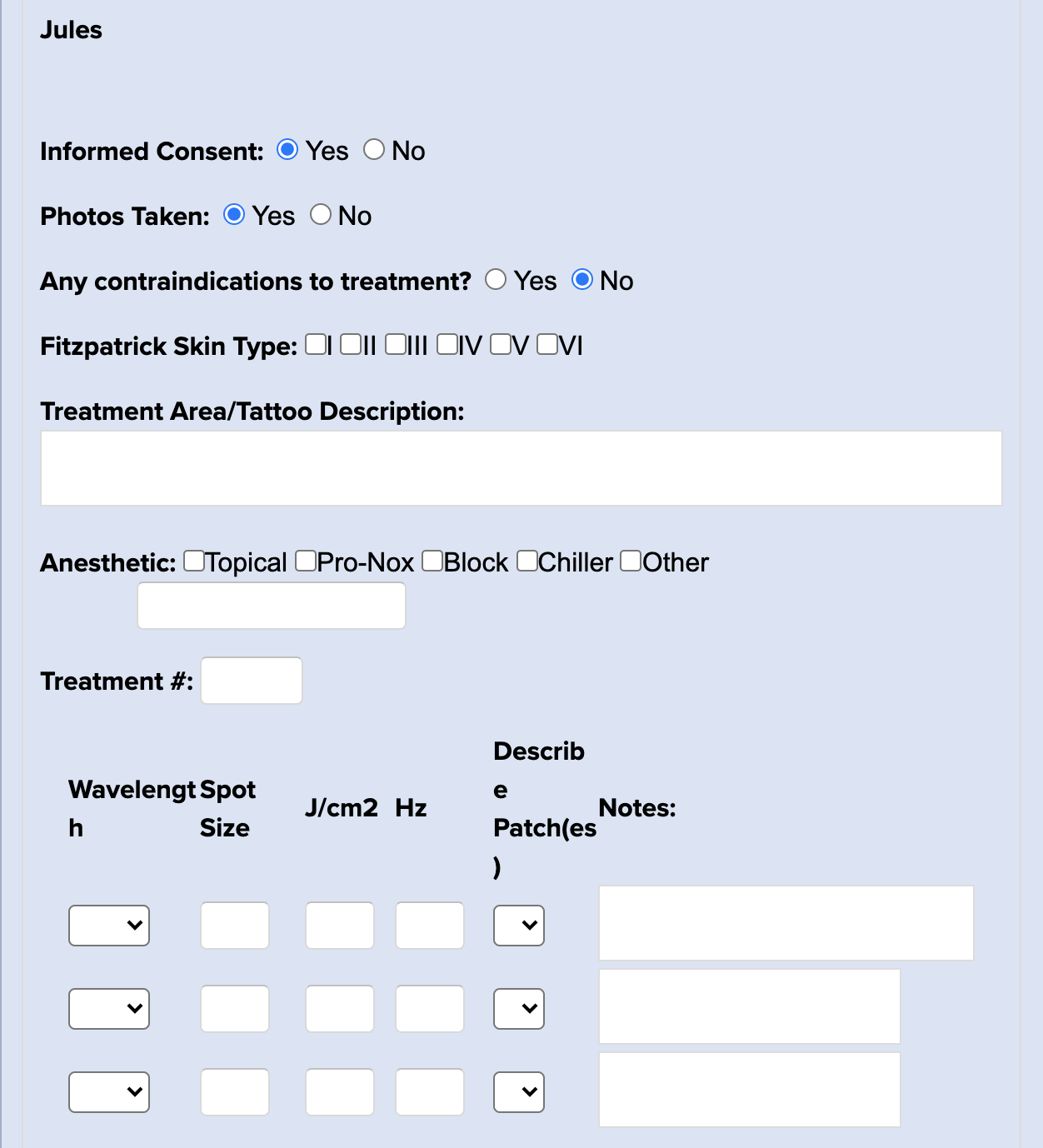
Laser Tattoo Removal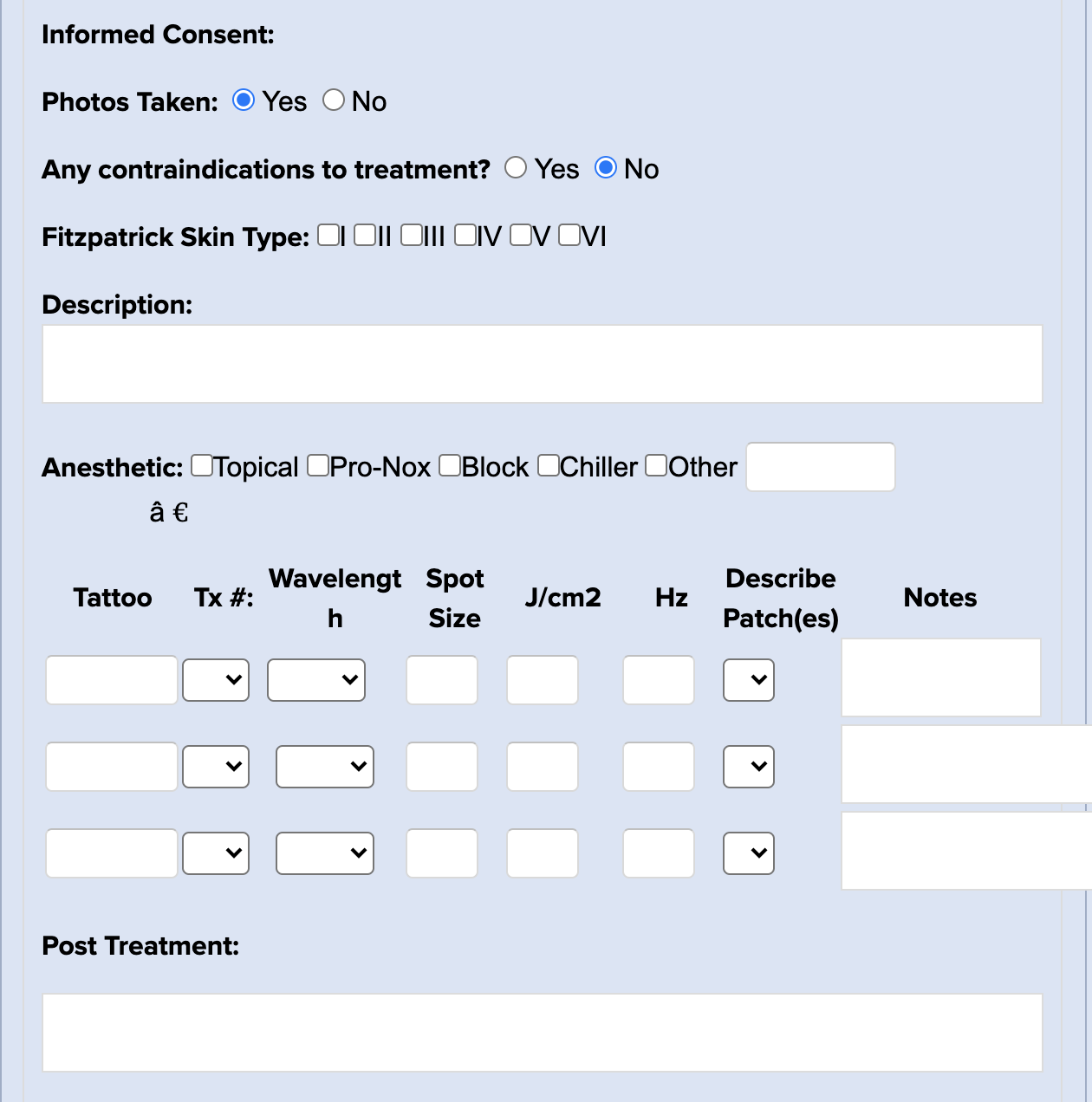
Lip Lift
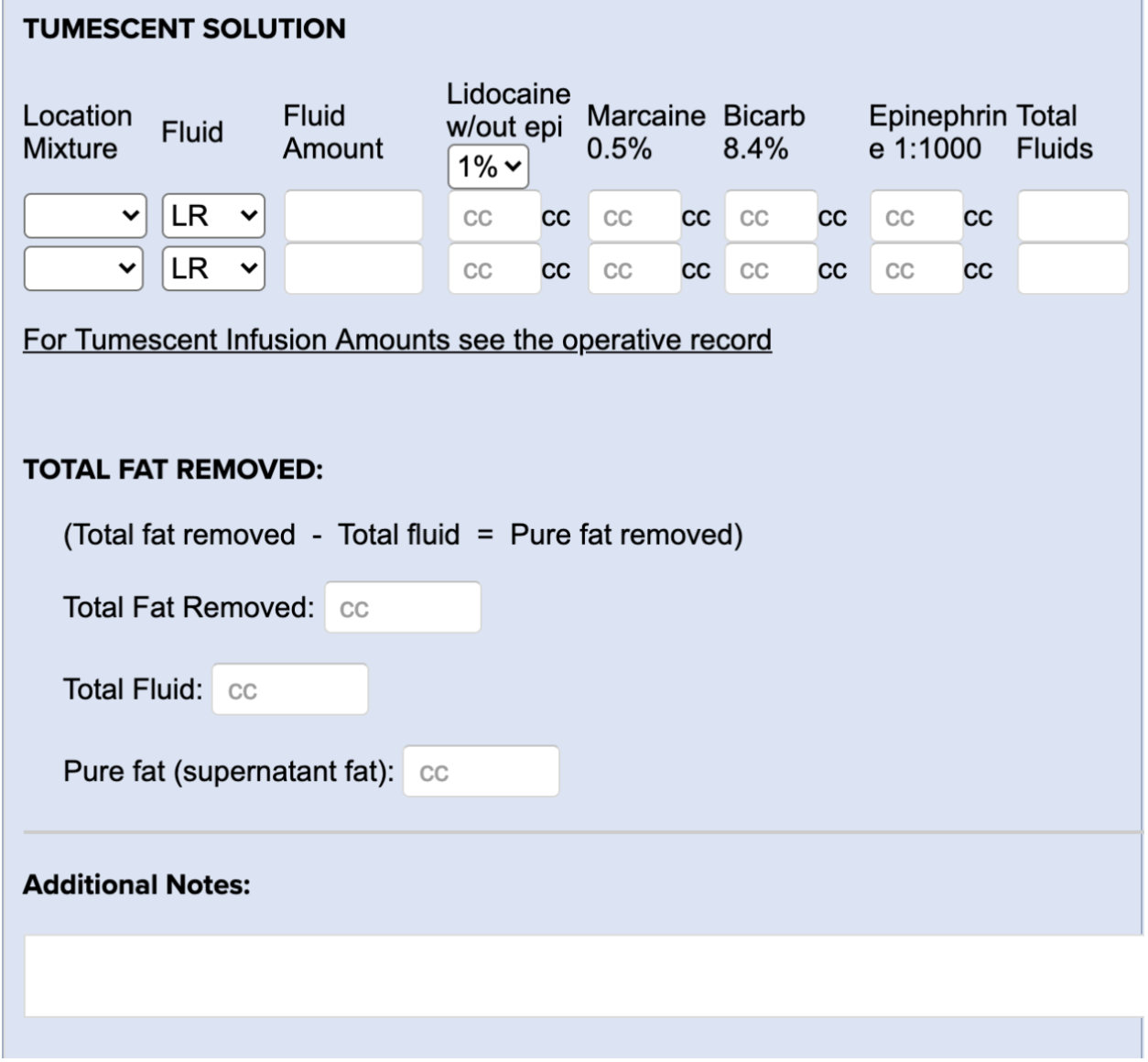
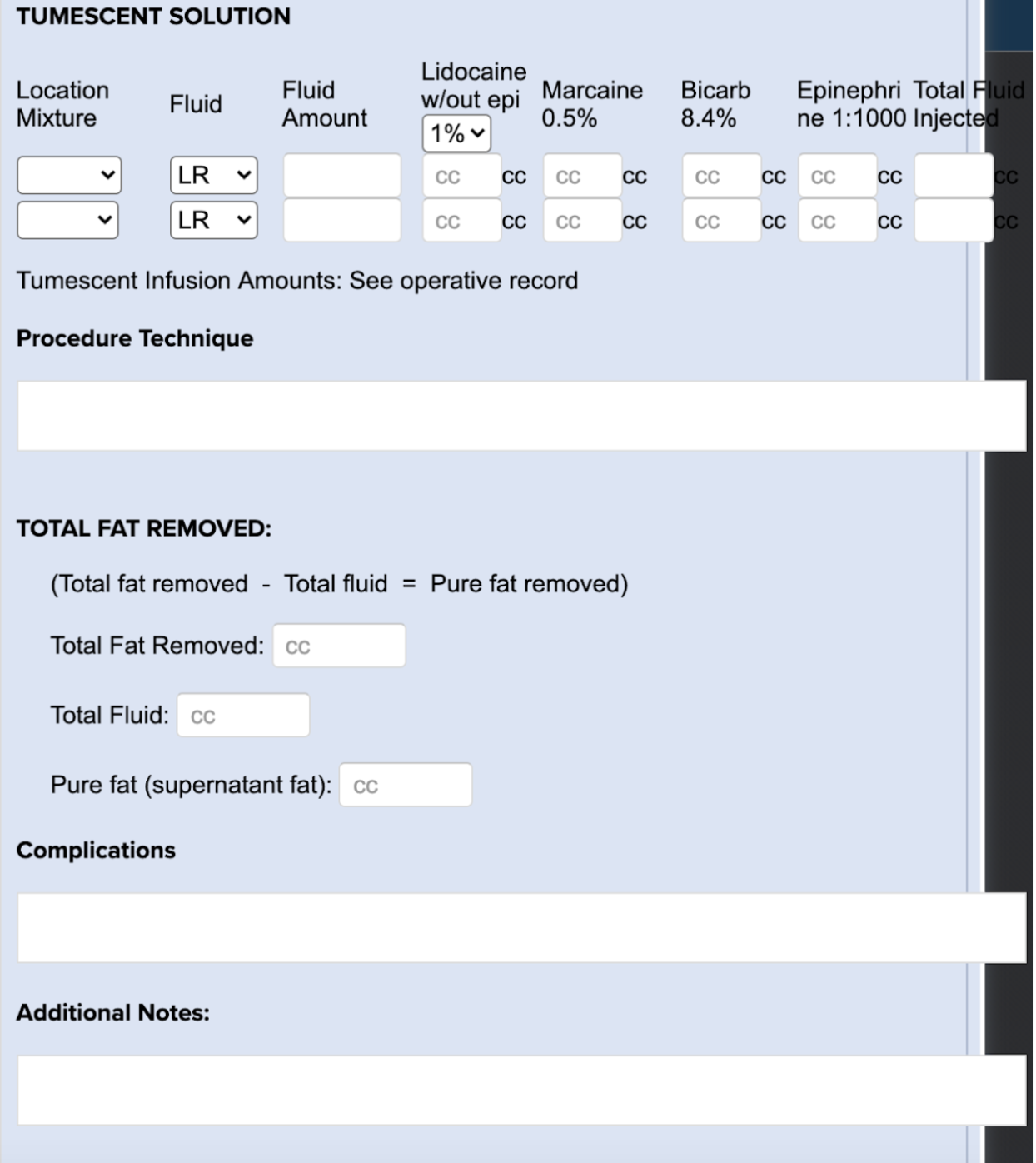
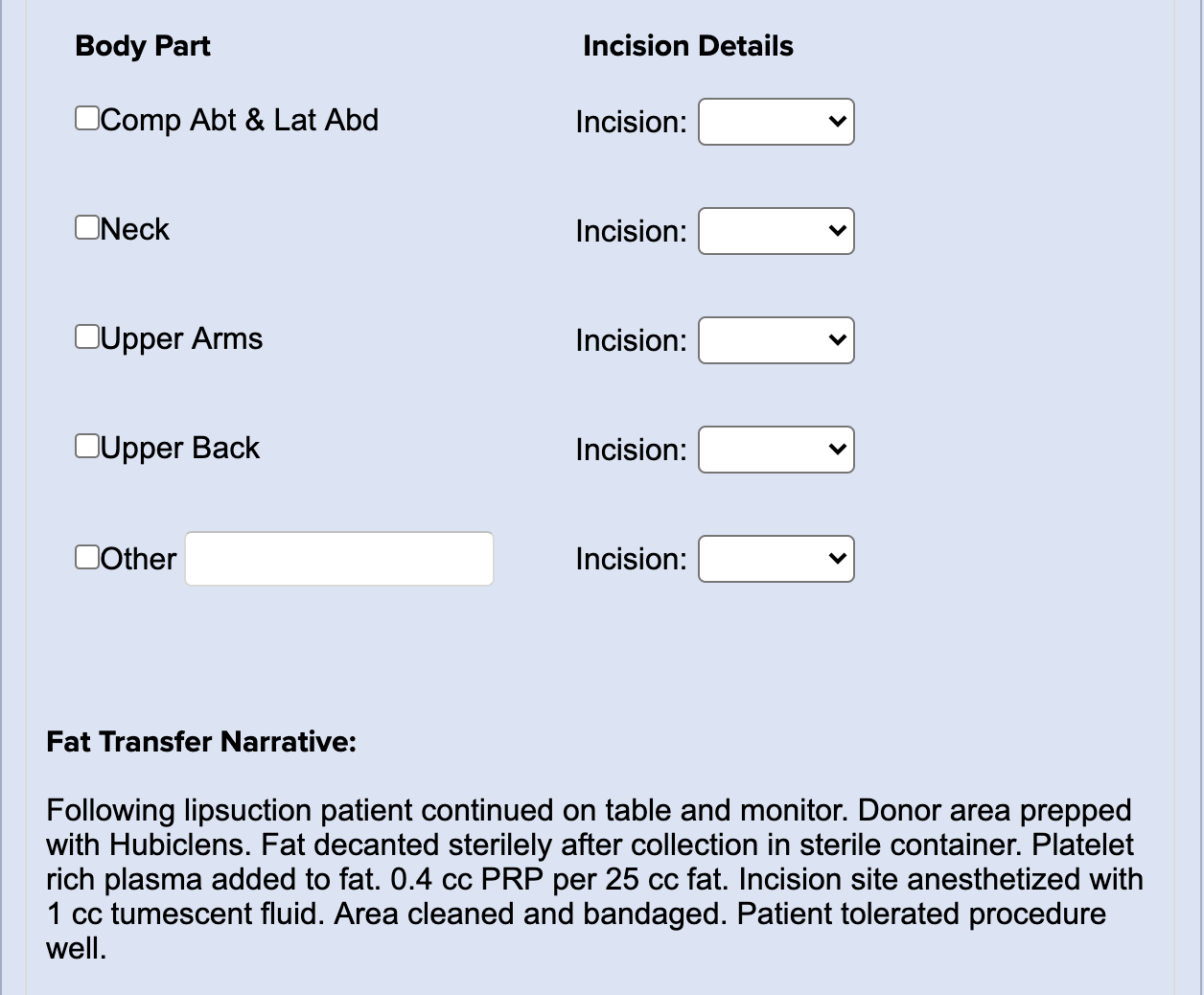
Liposuction + Fat Transfer
Microneeding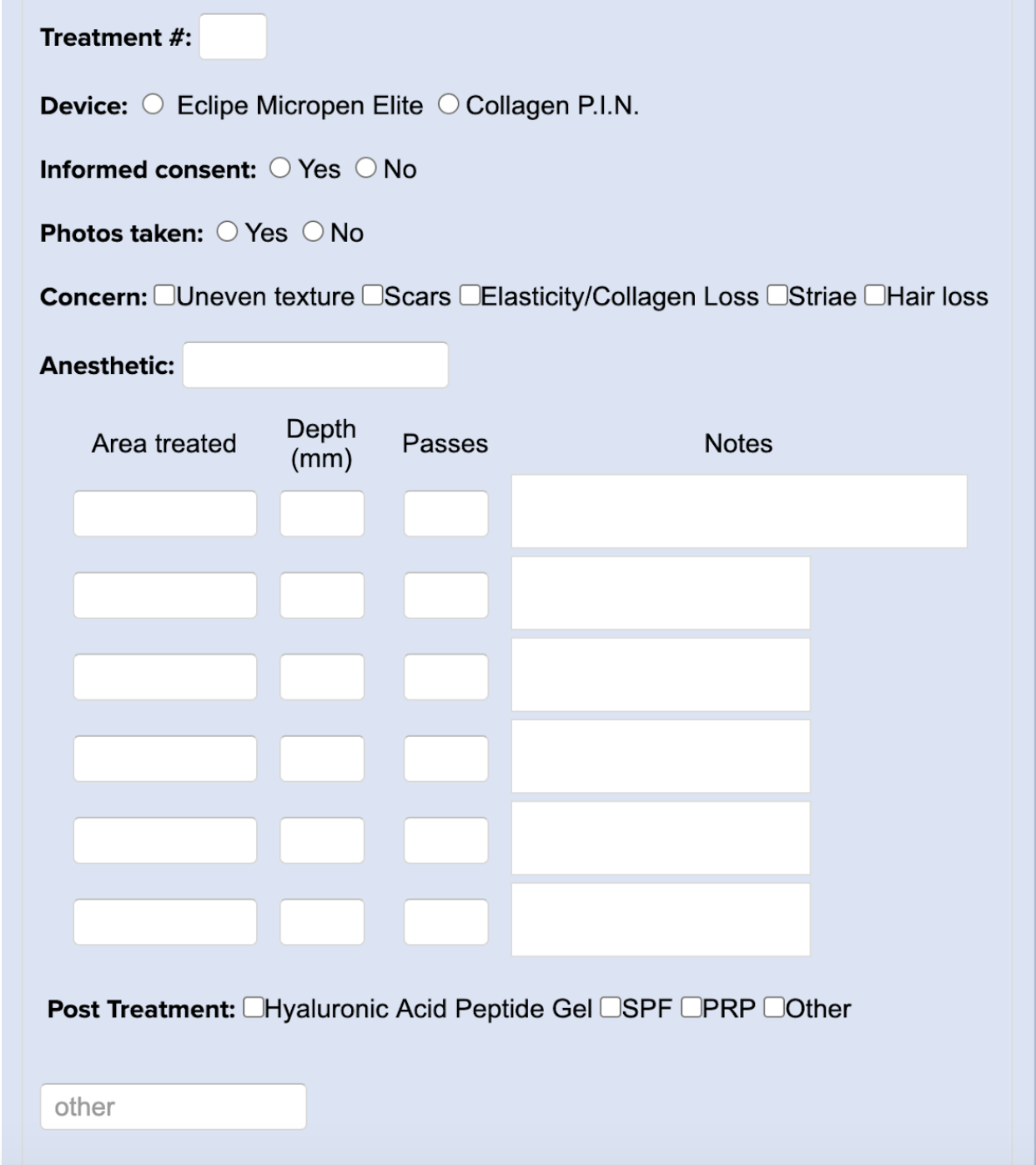
Neurotoxins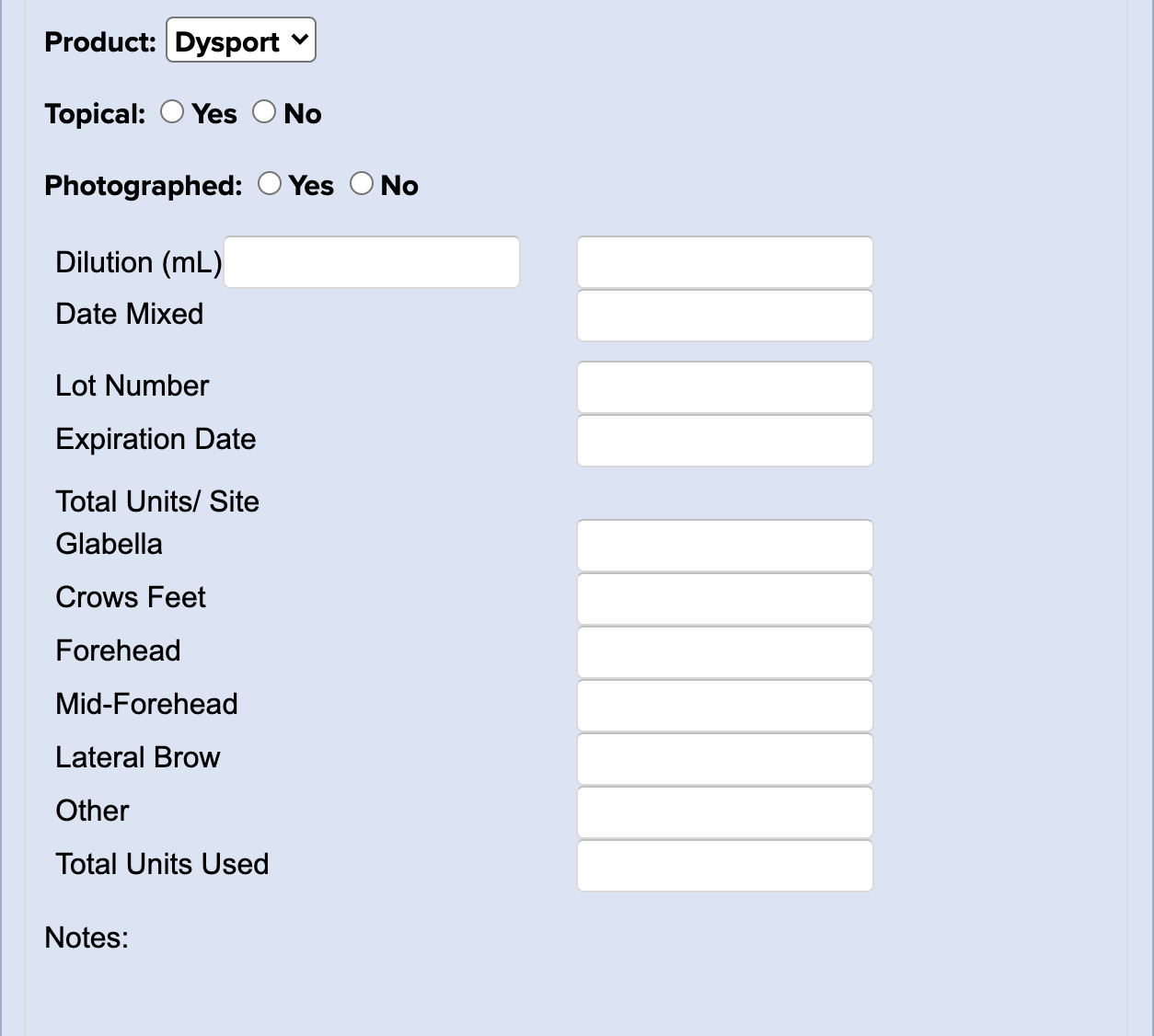
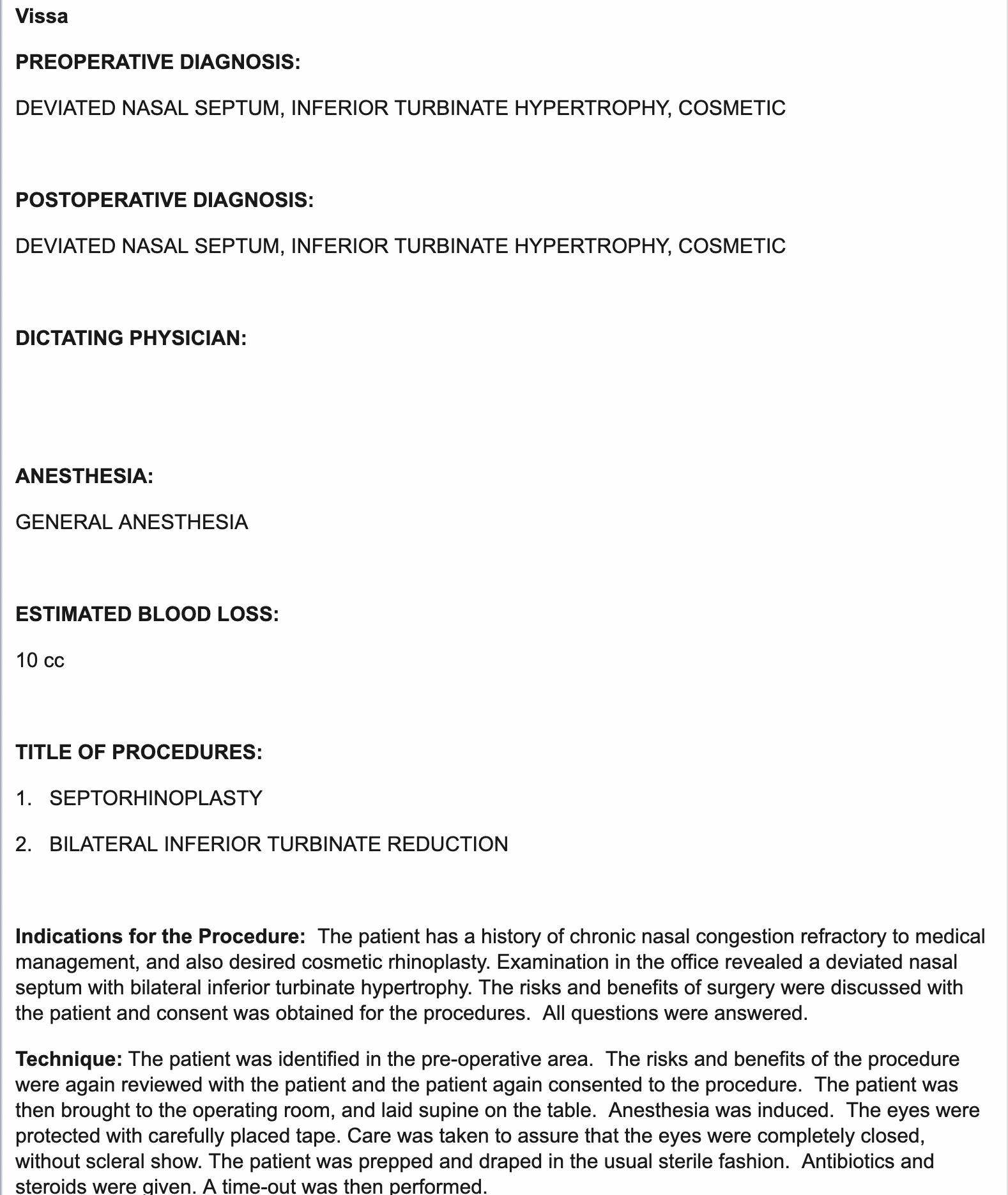
Open Rhinoplasty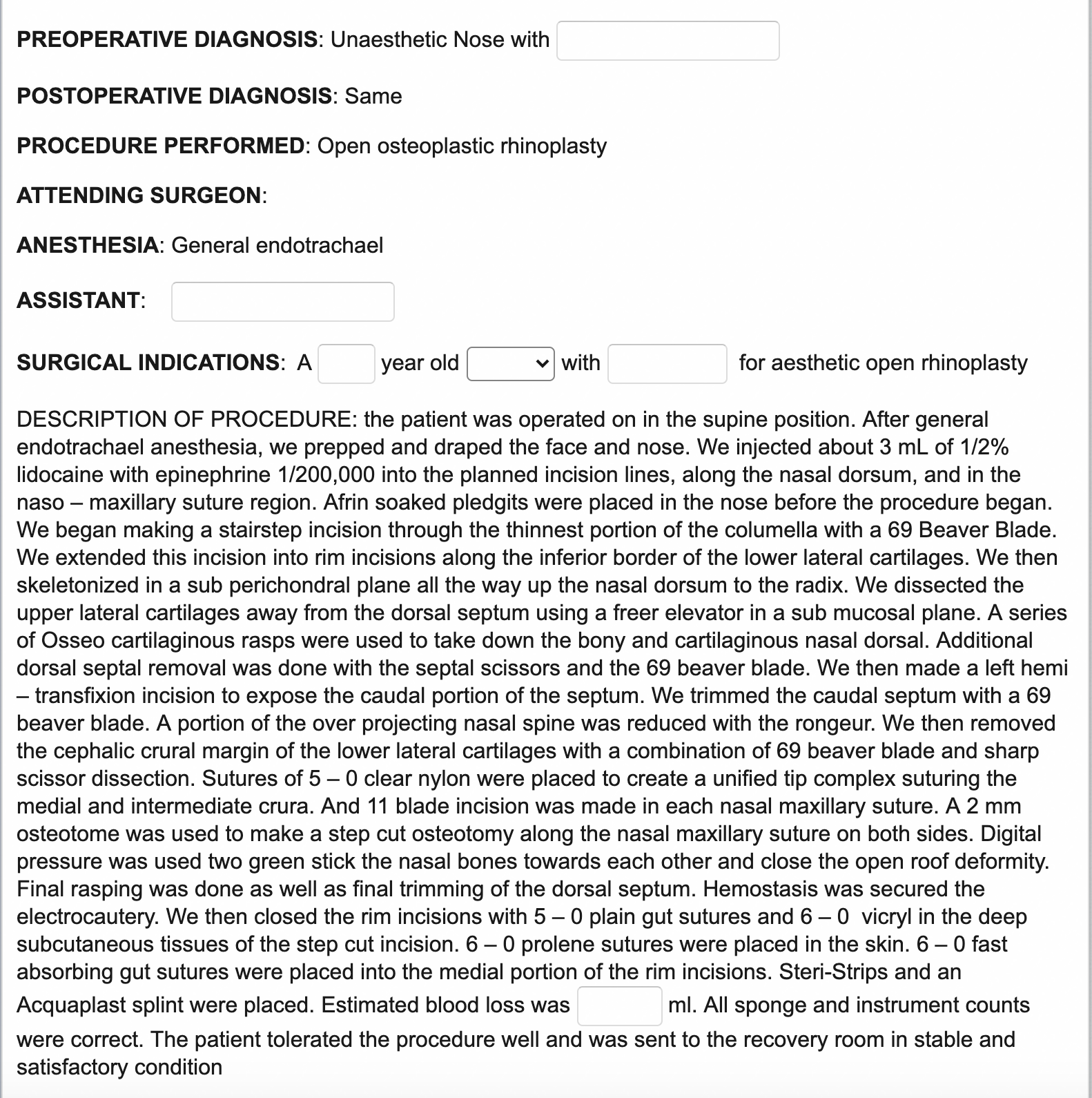
Operative Notes
Pellet Insertion
Pre-Operative Appointment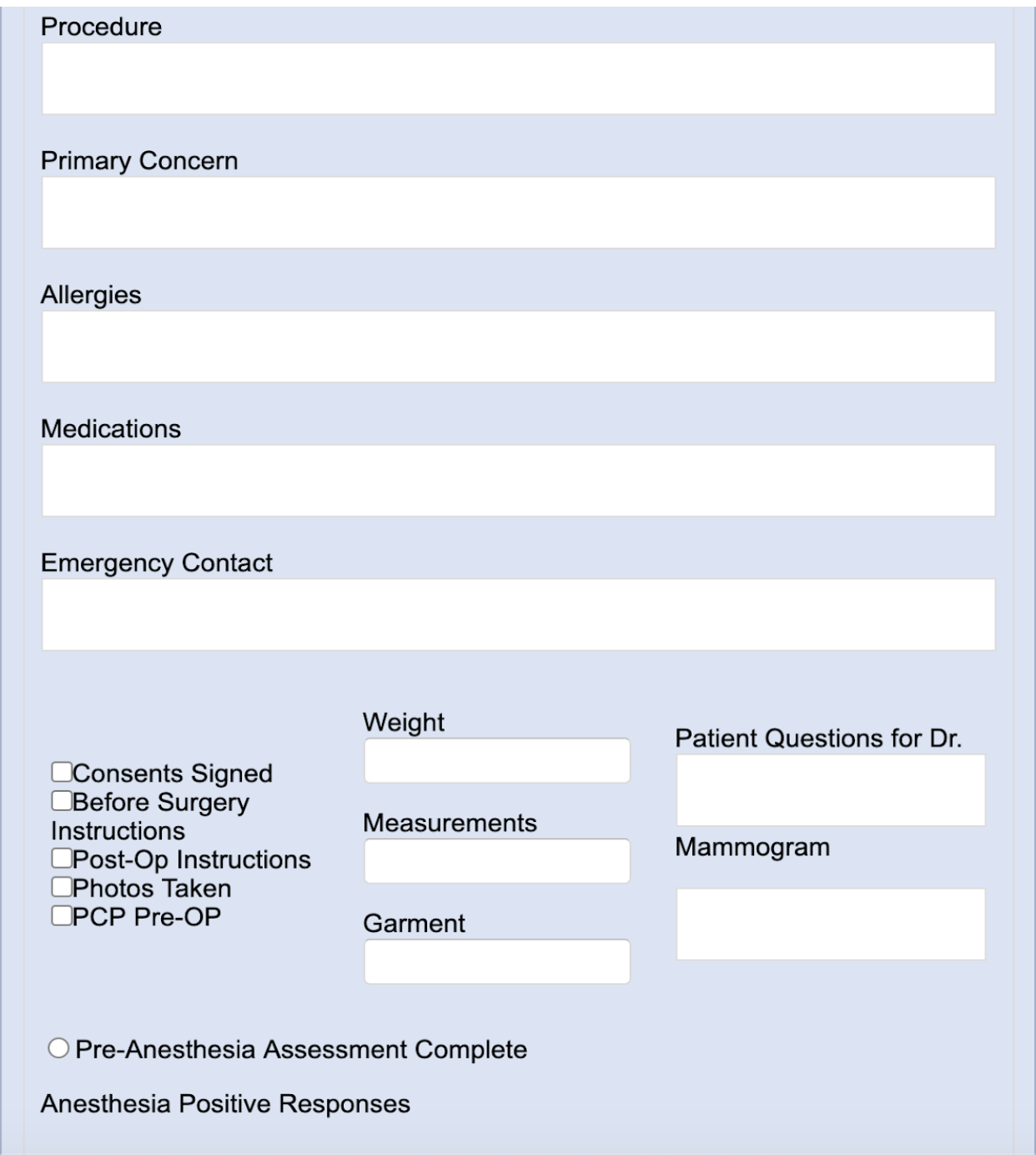
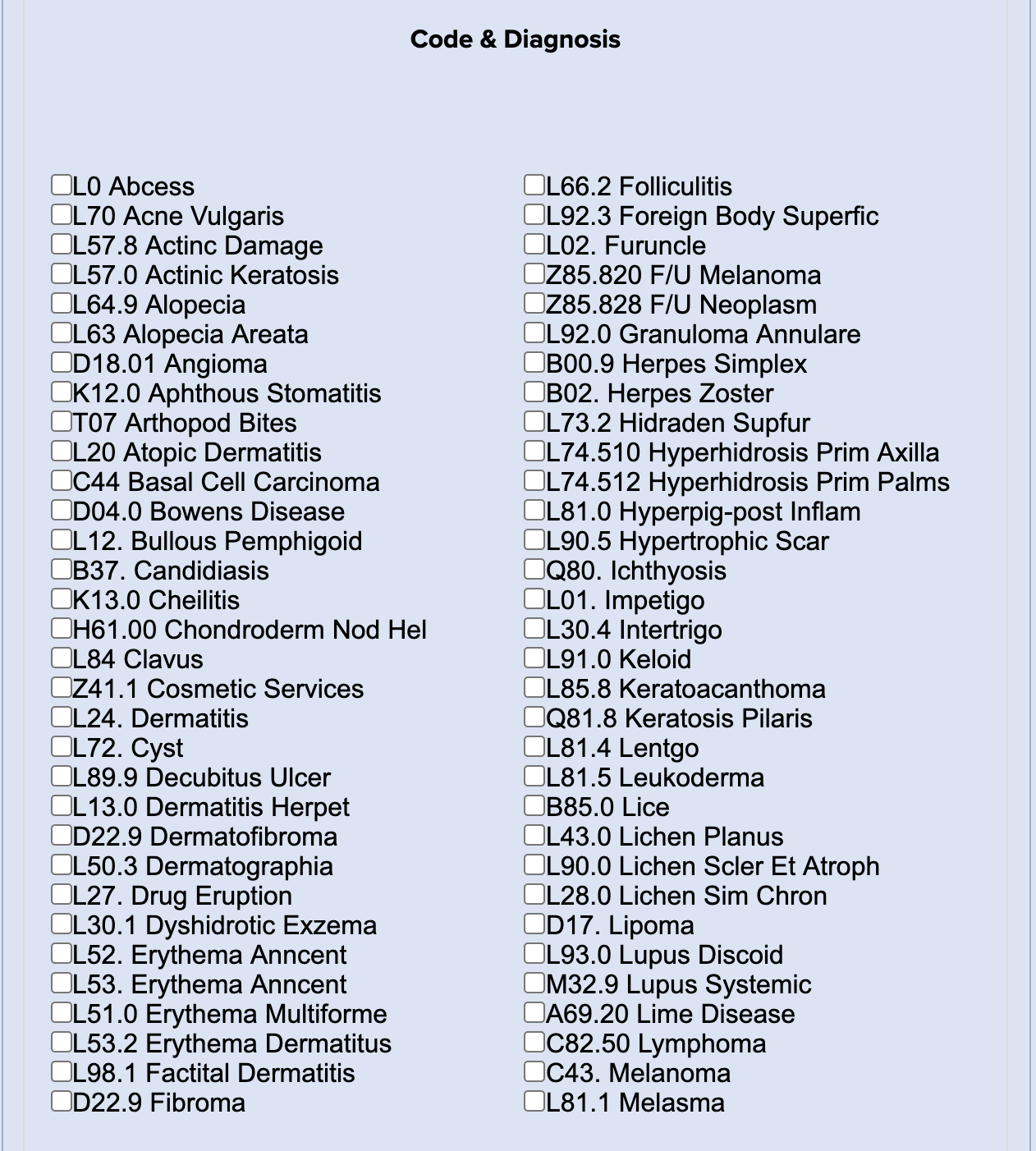
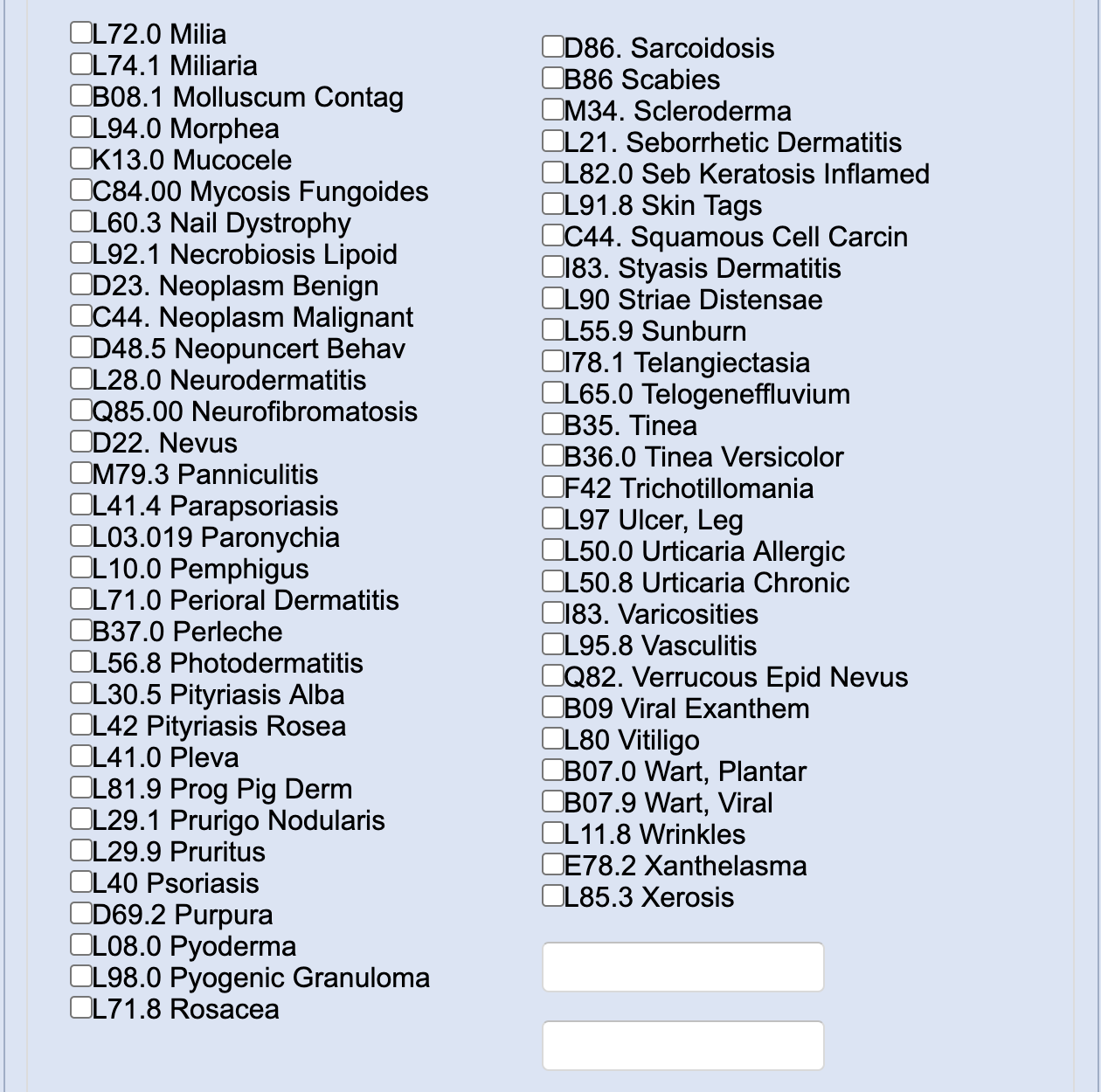
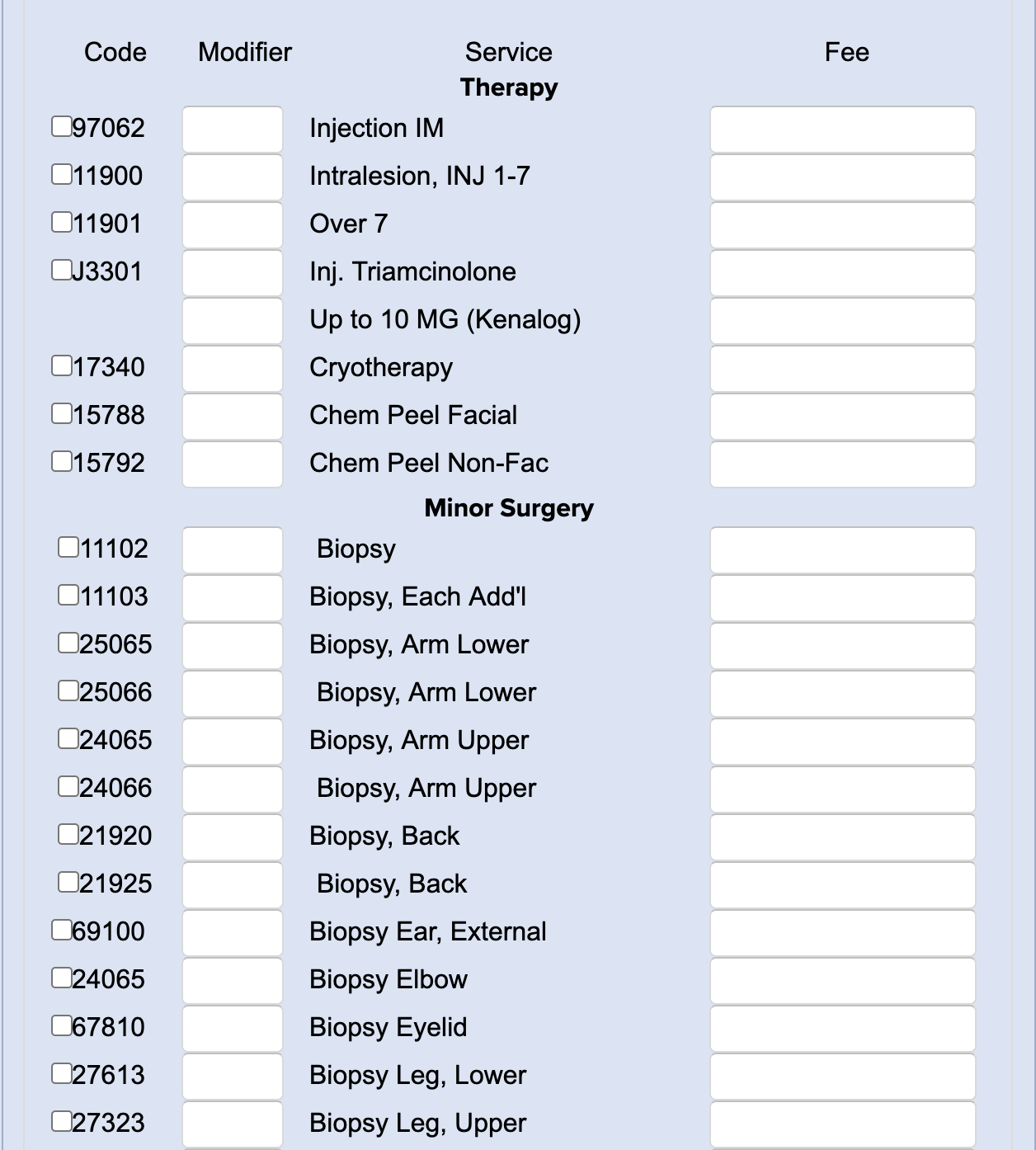
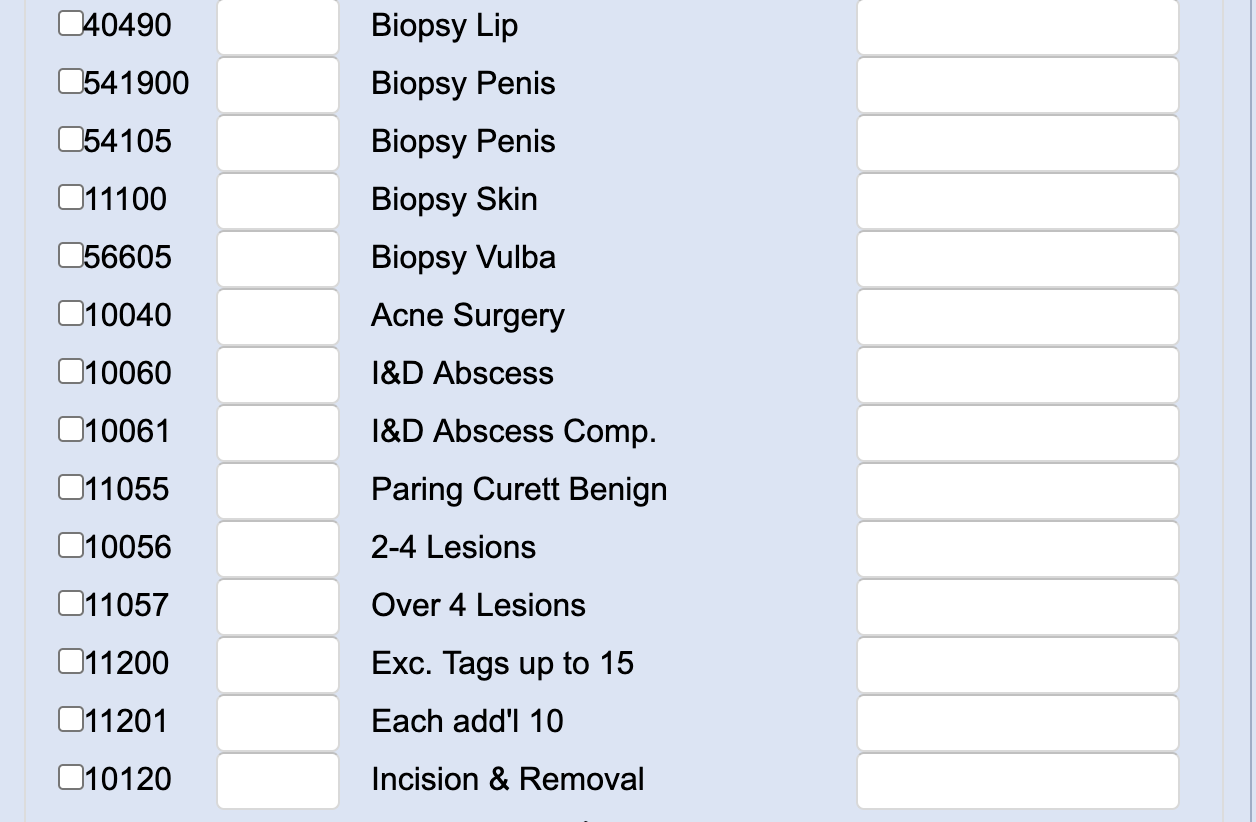
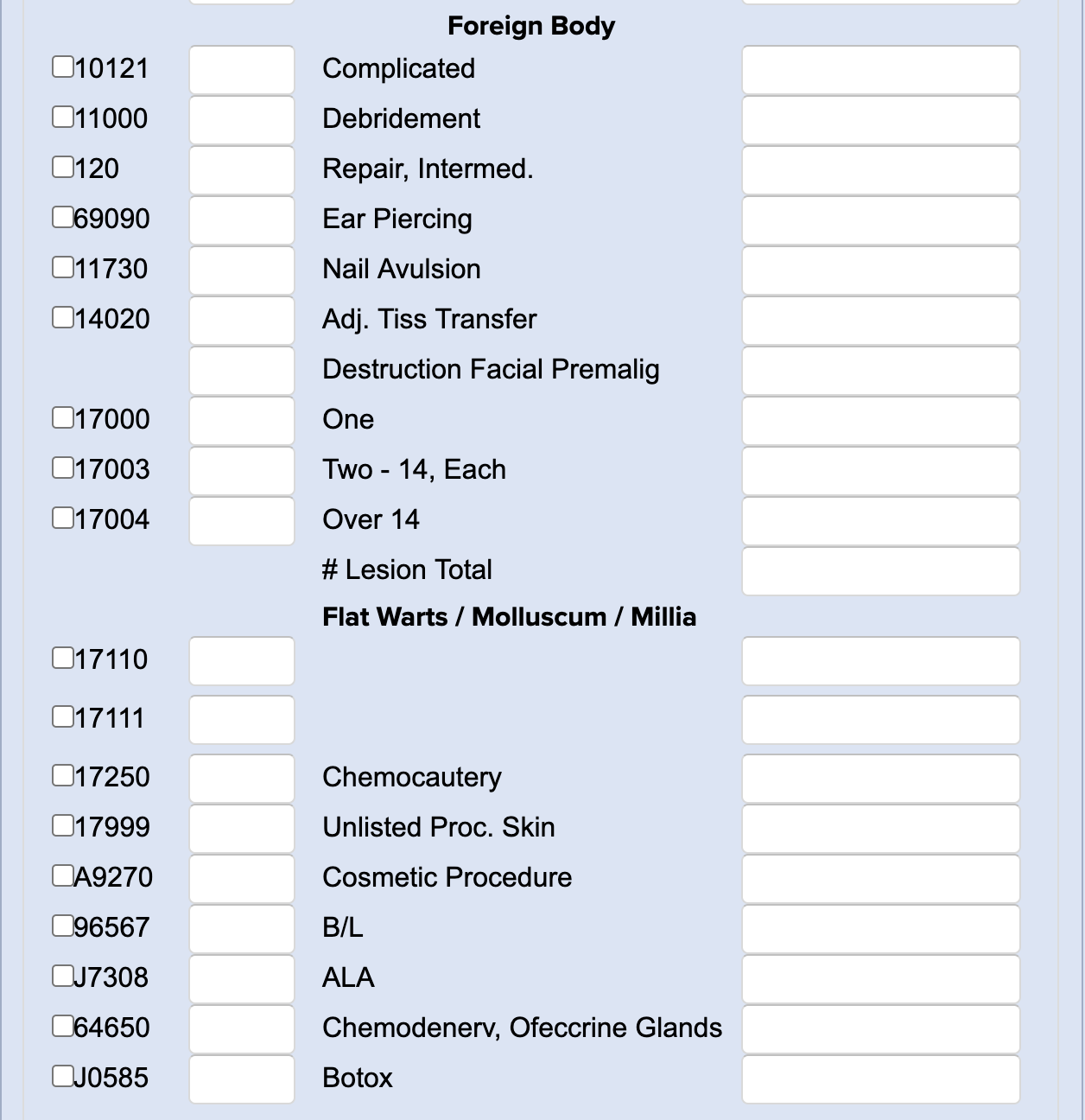
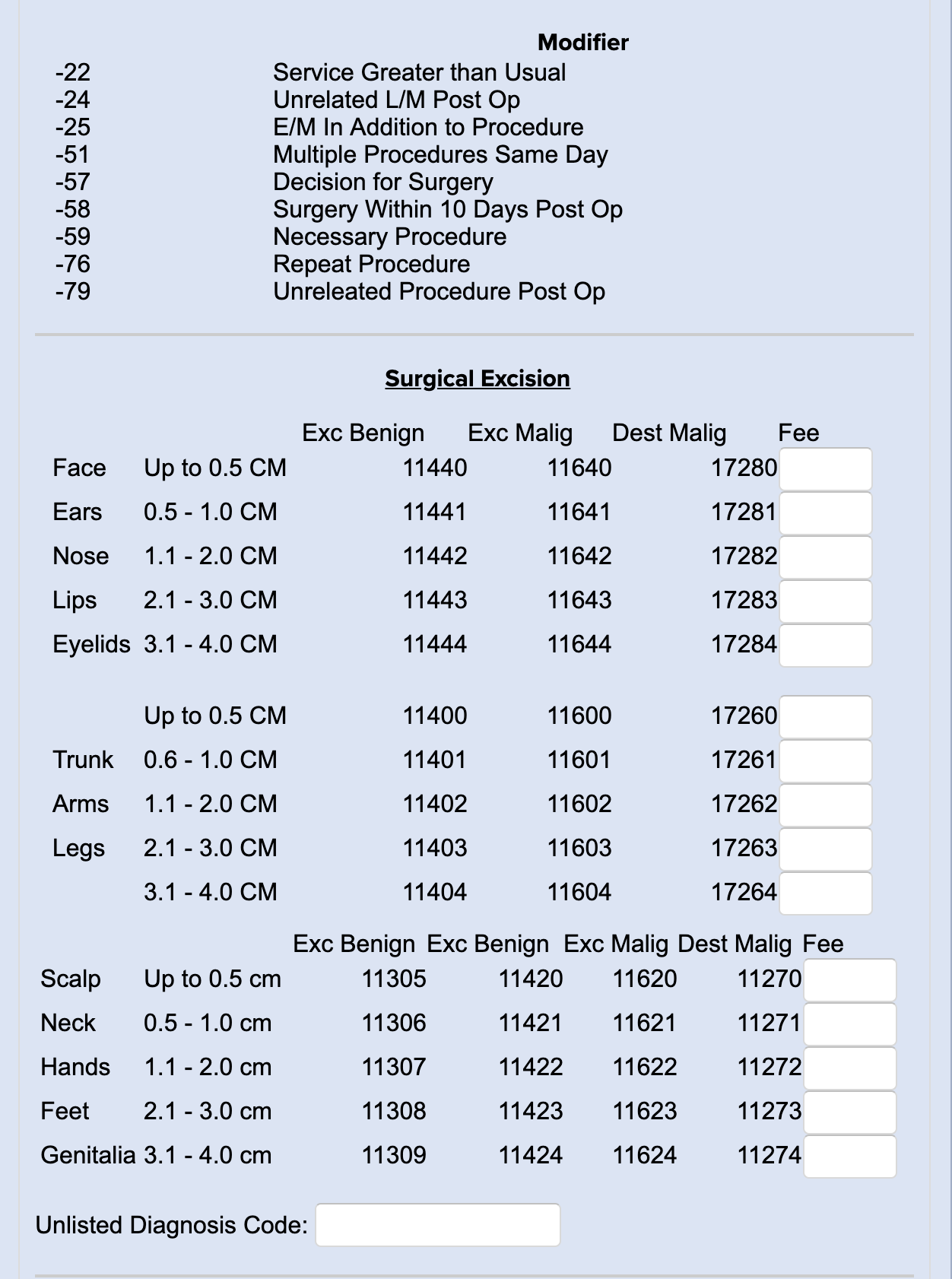
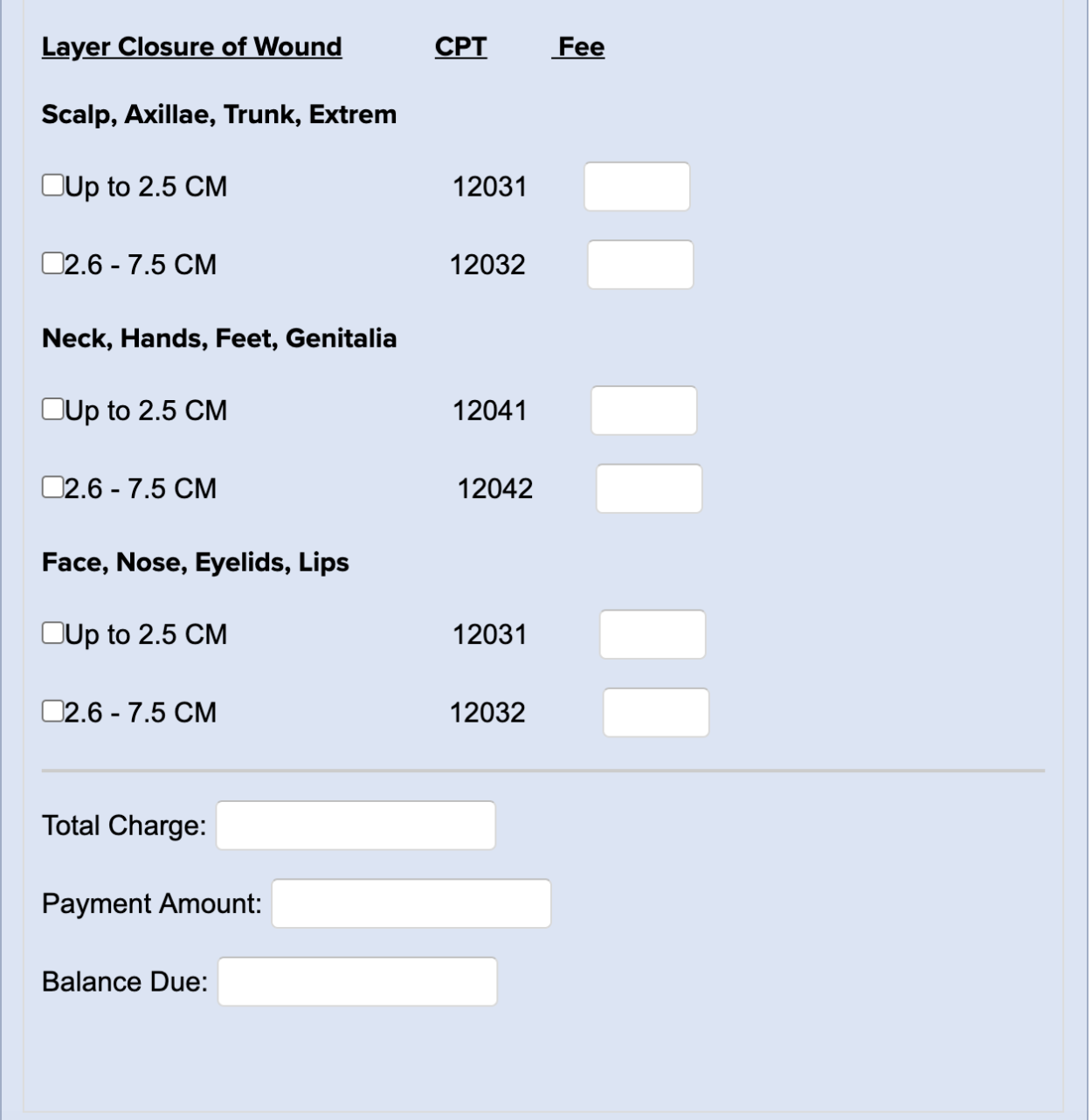
Sample Superbill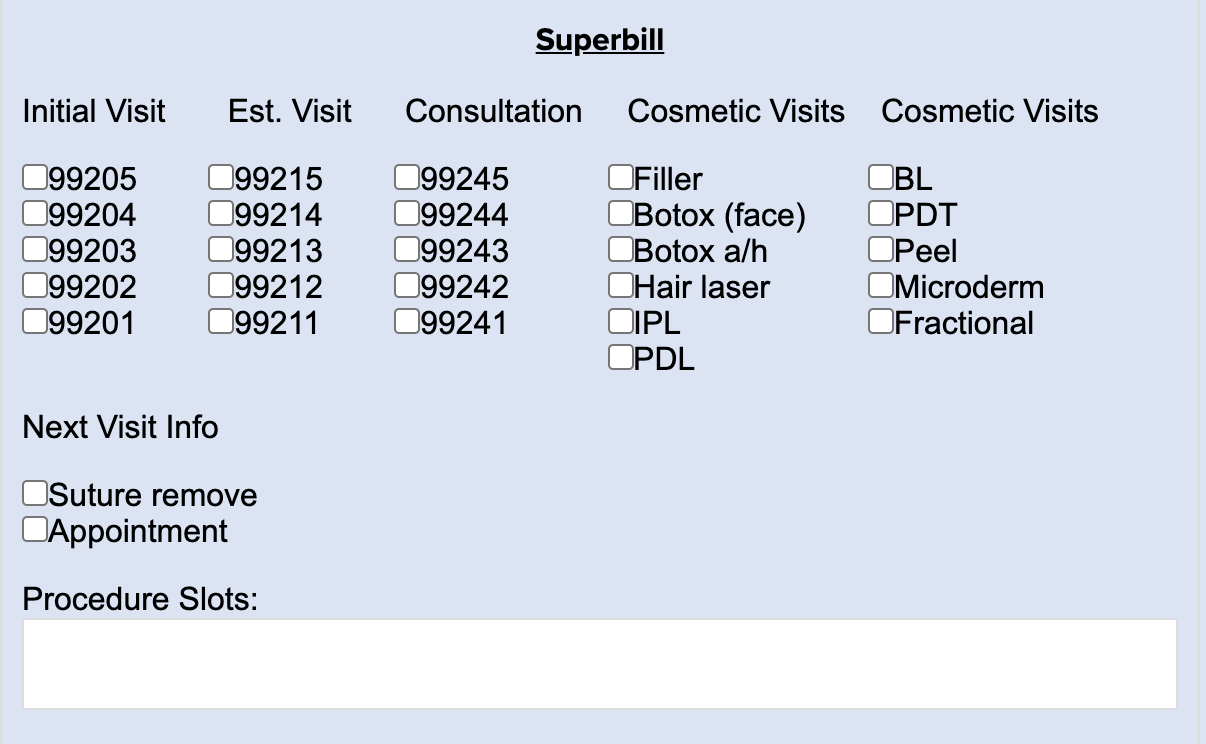
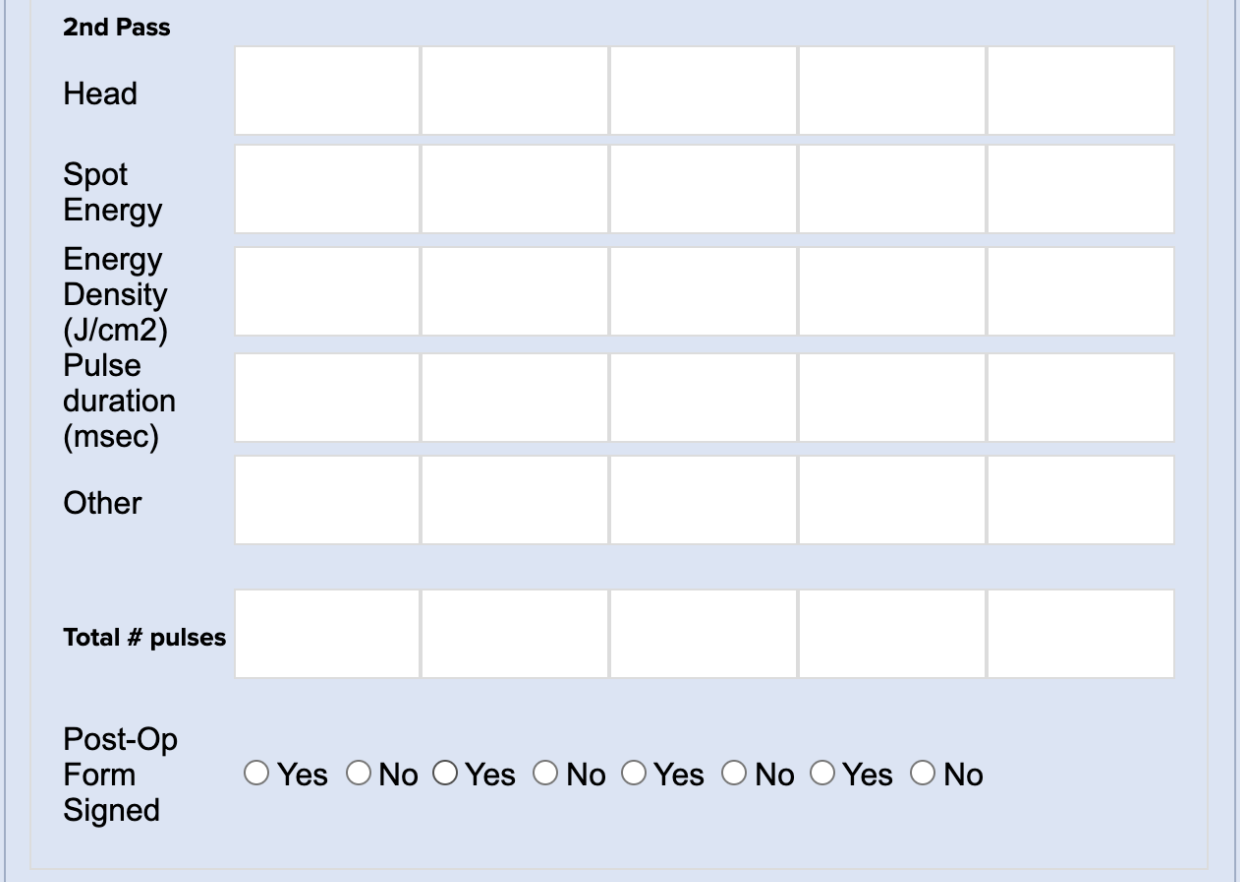
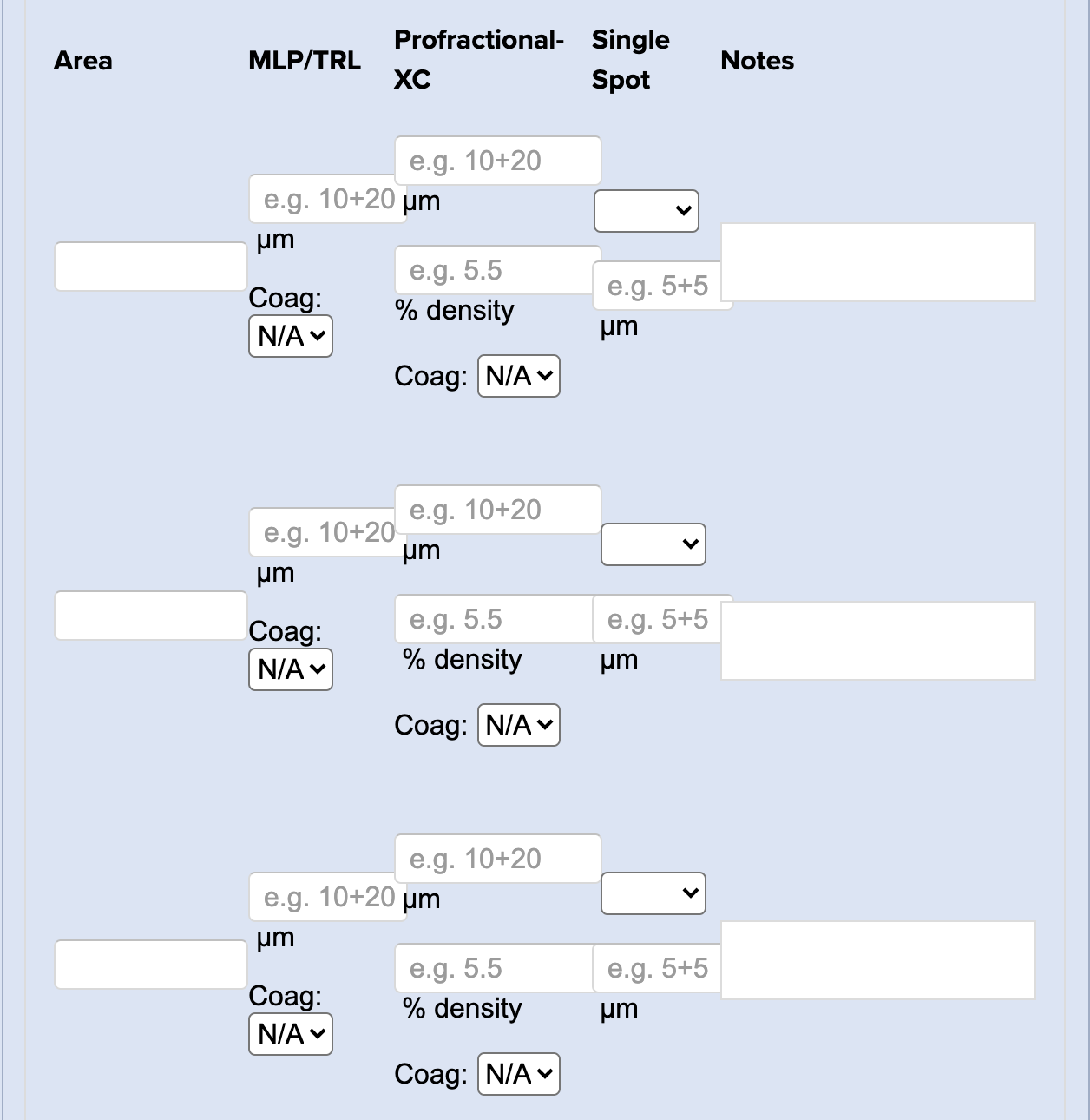
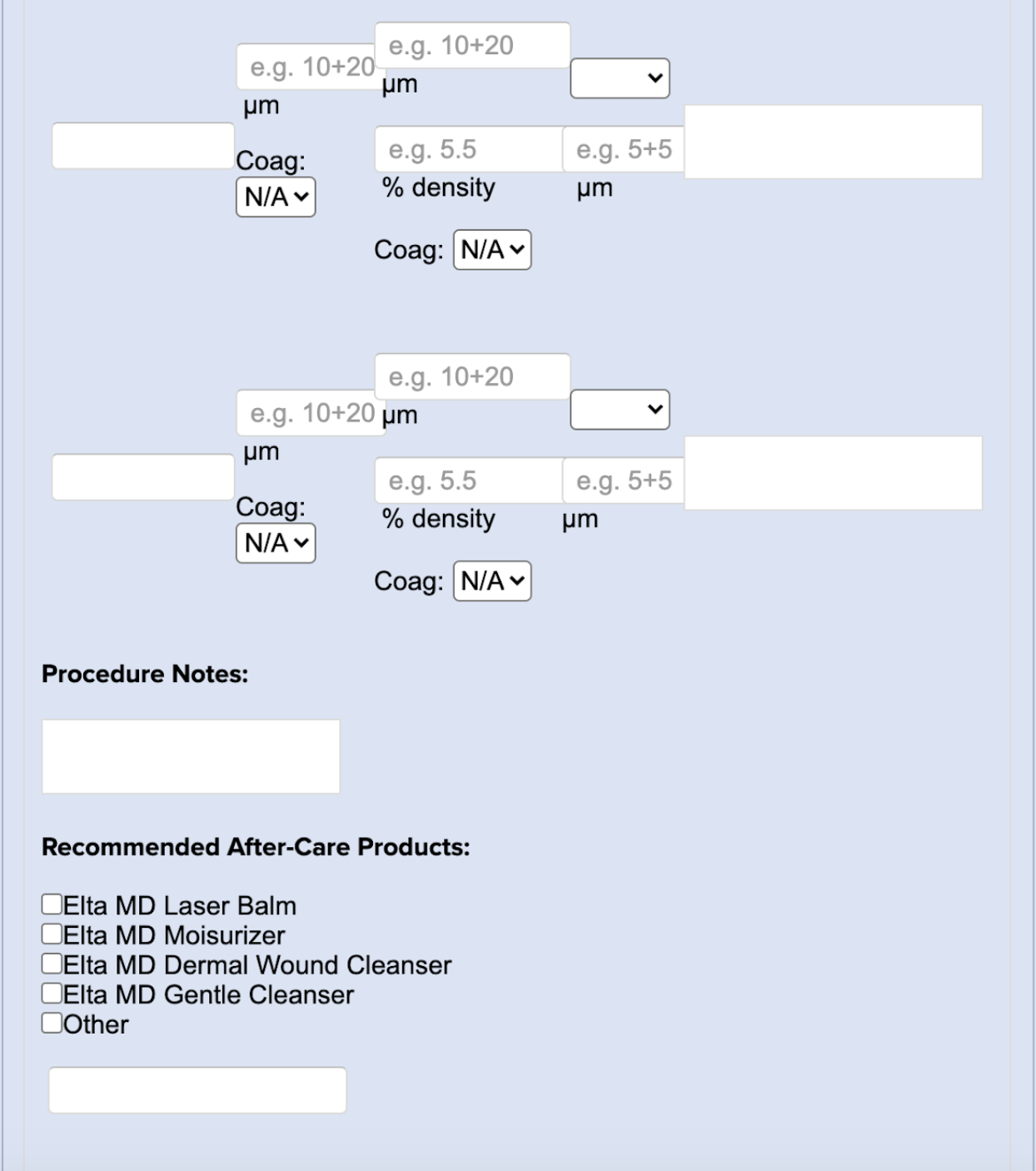
Sciton Erbium Laser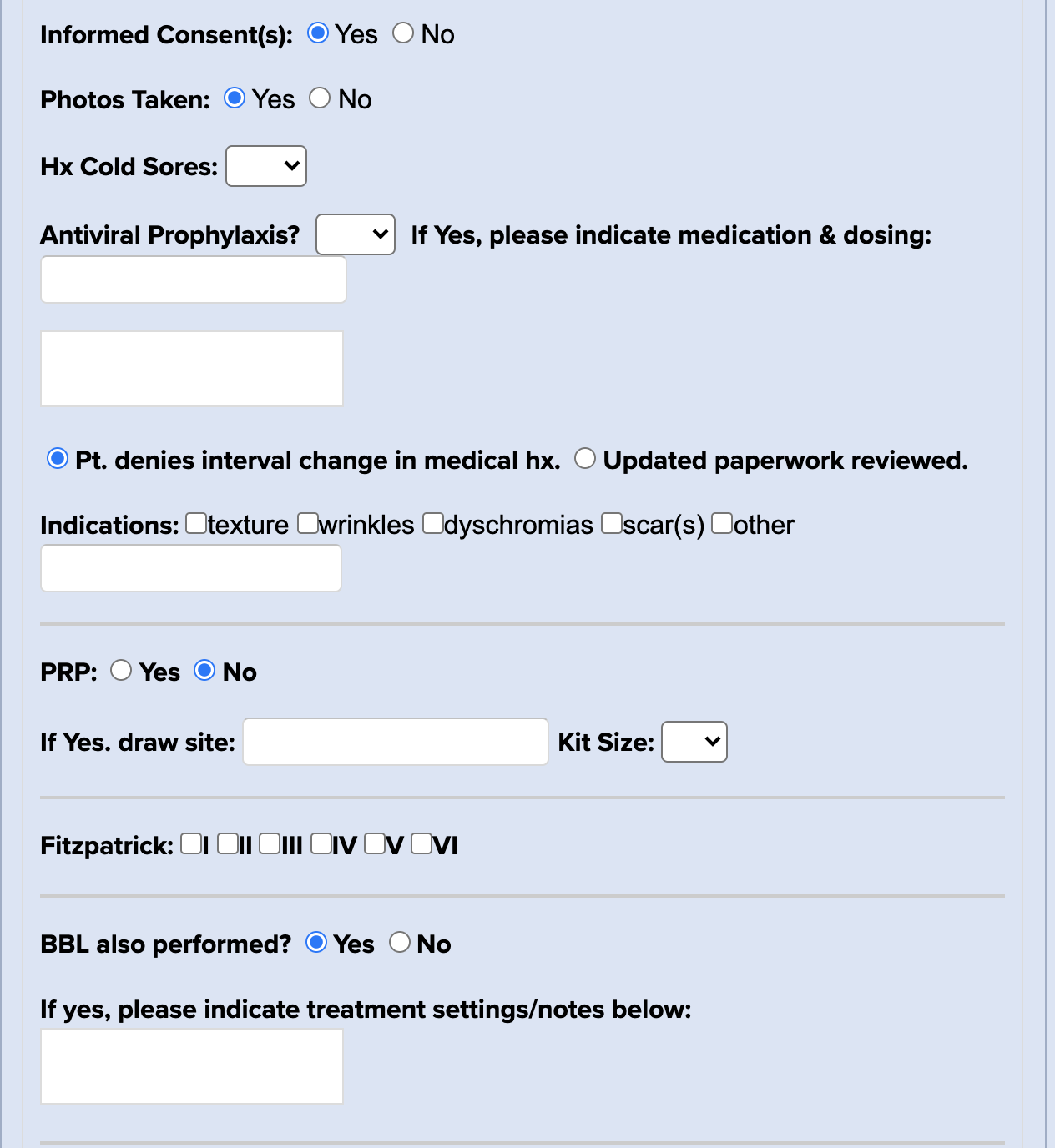
Sculptra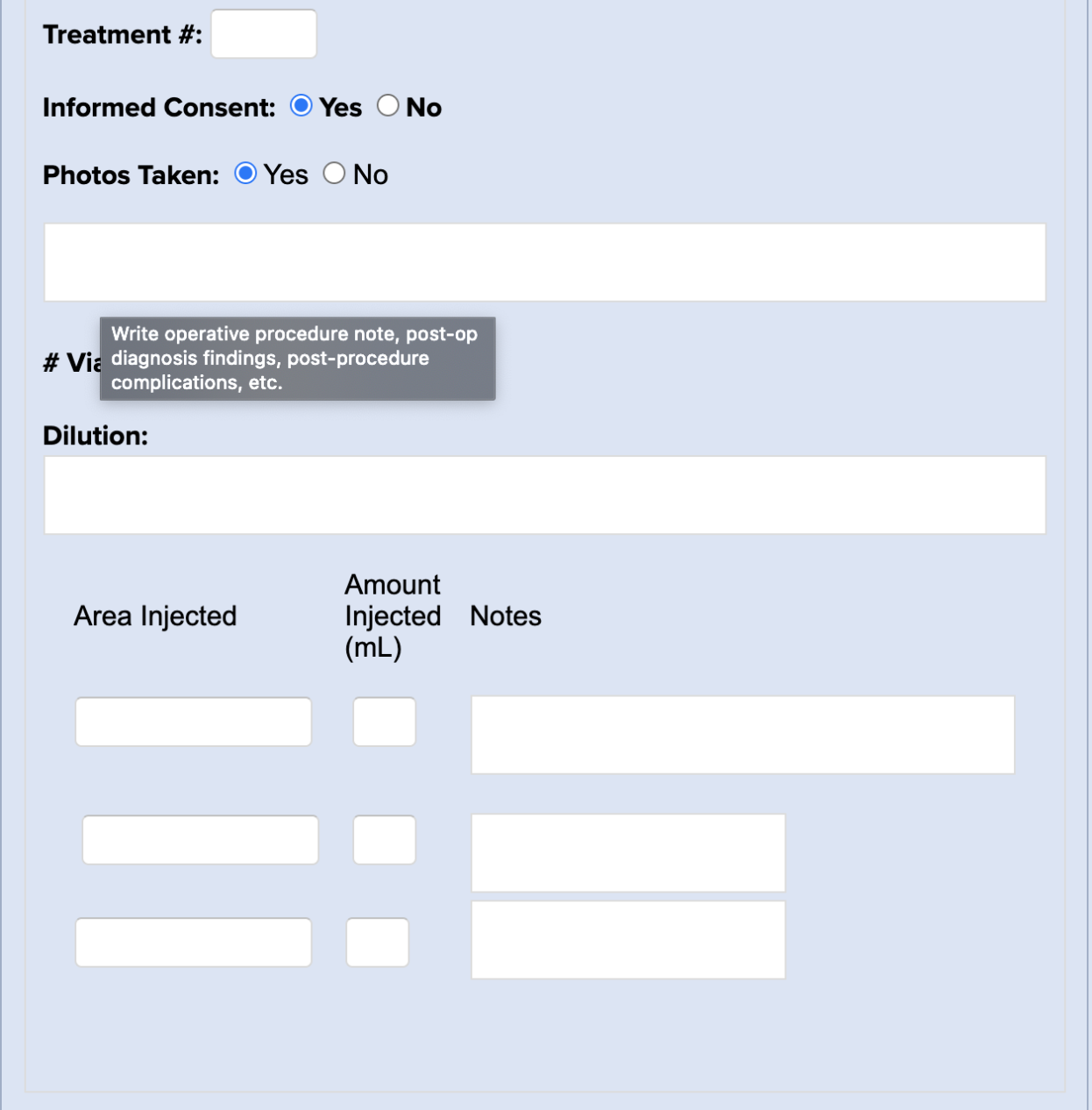
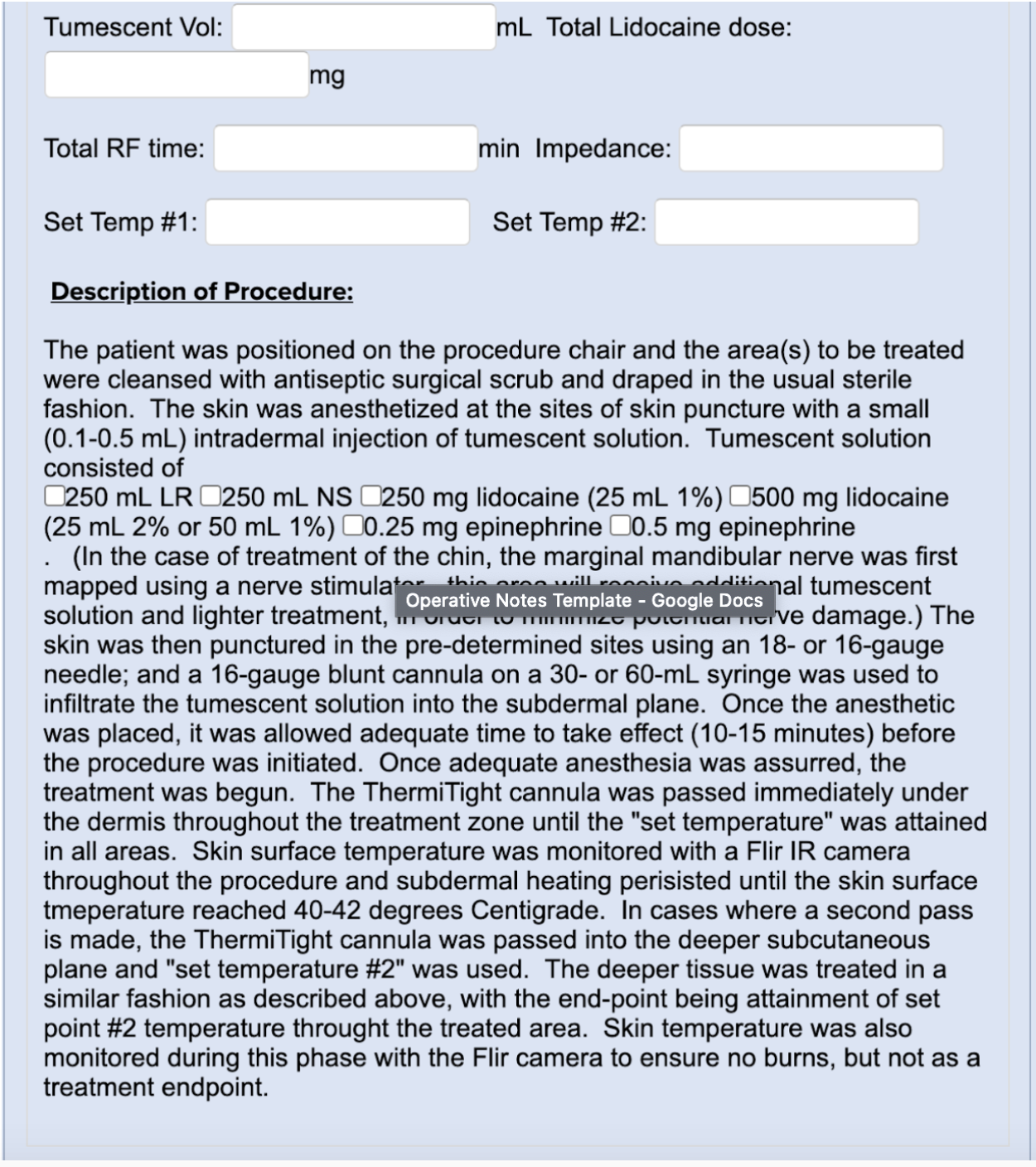
ThermiTight Treatment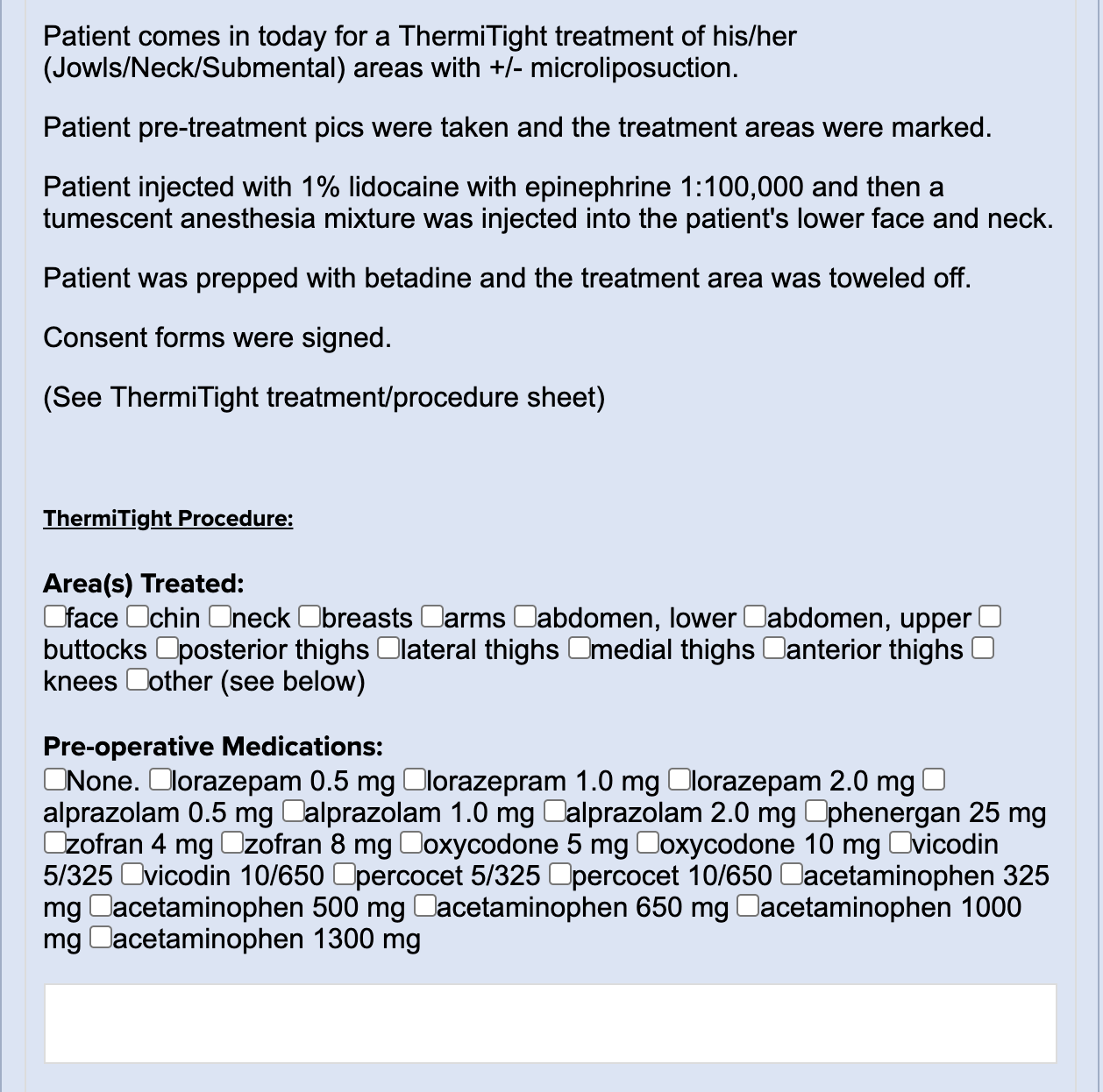
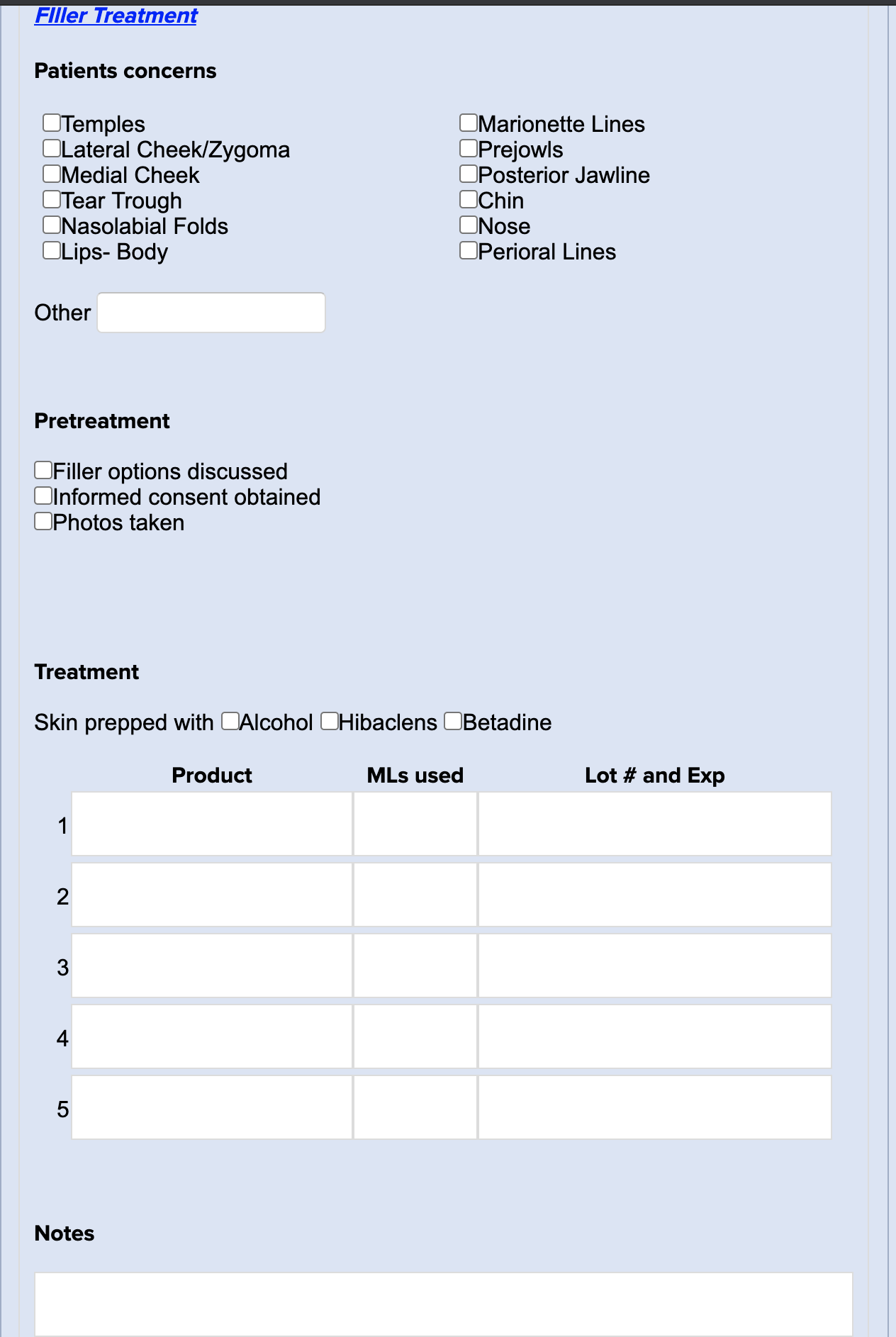
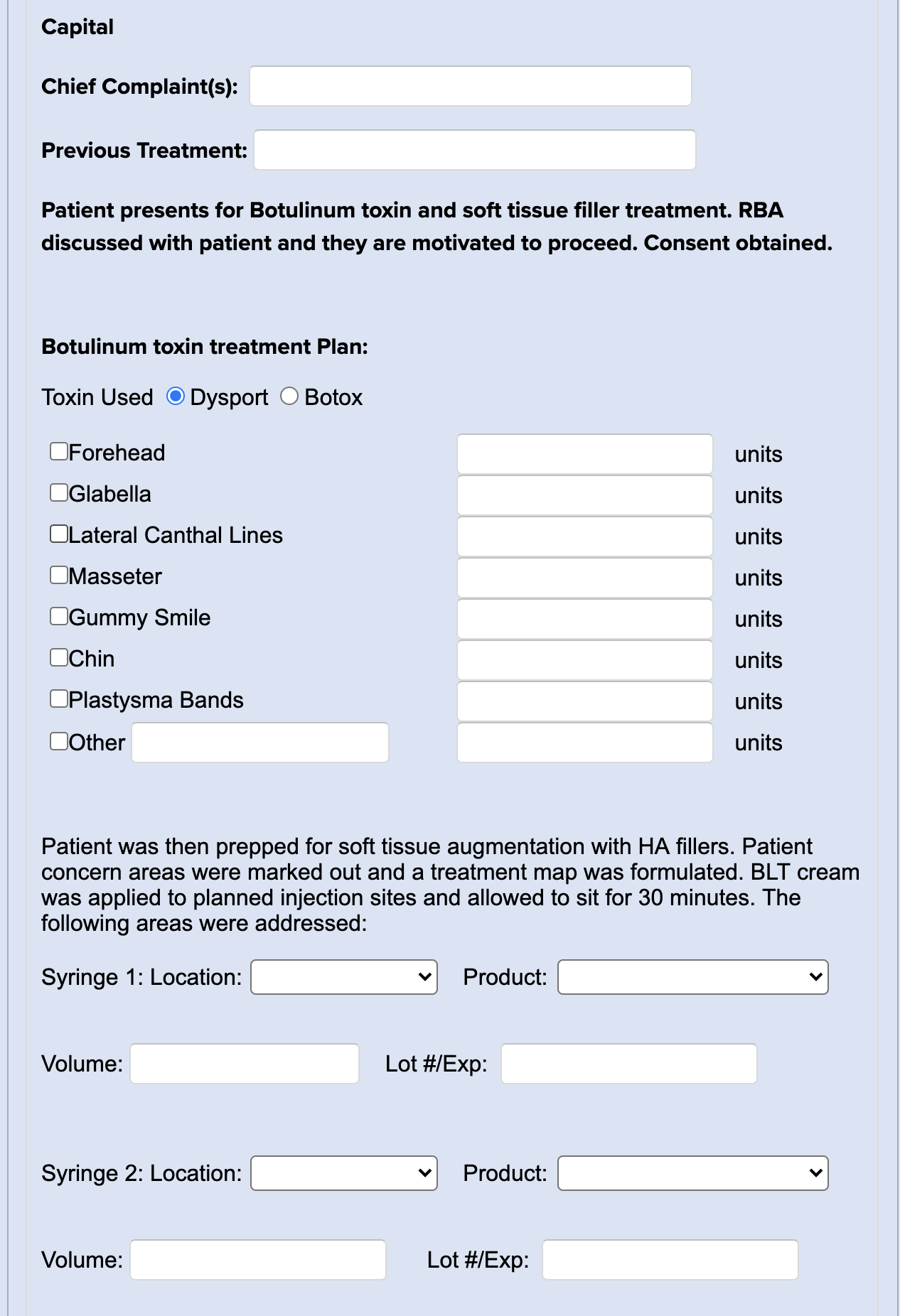
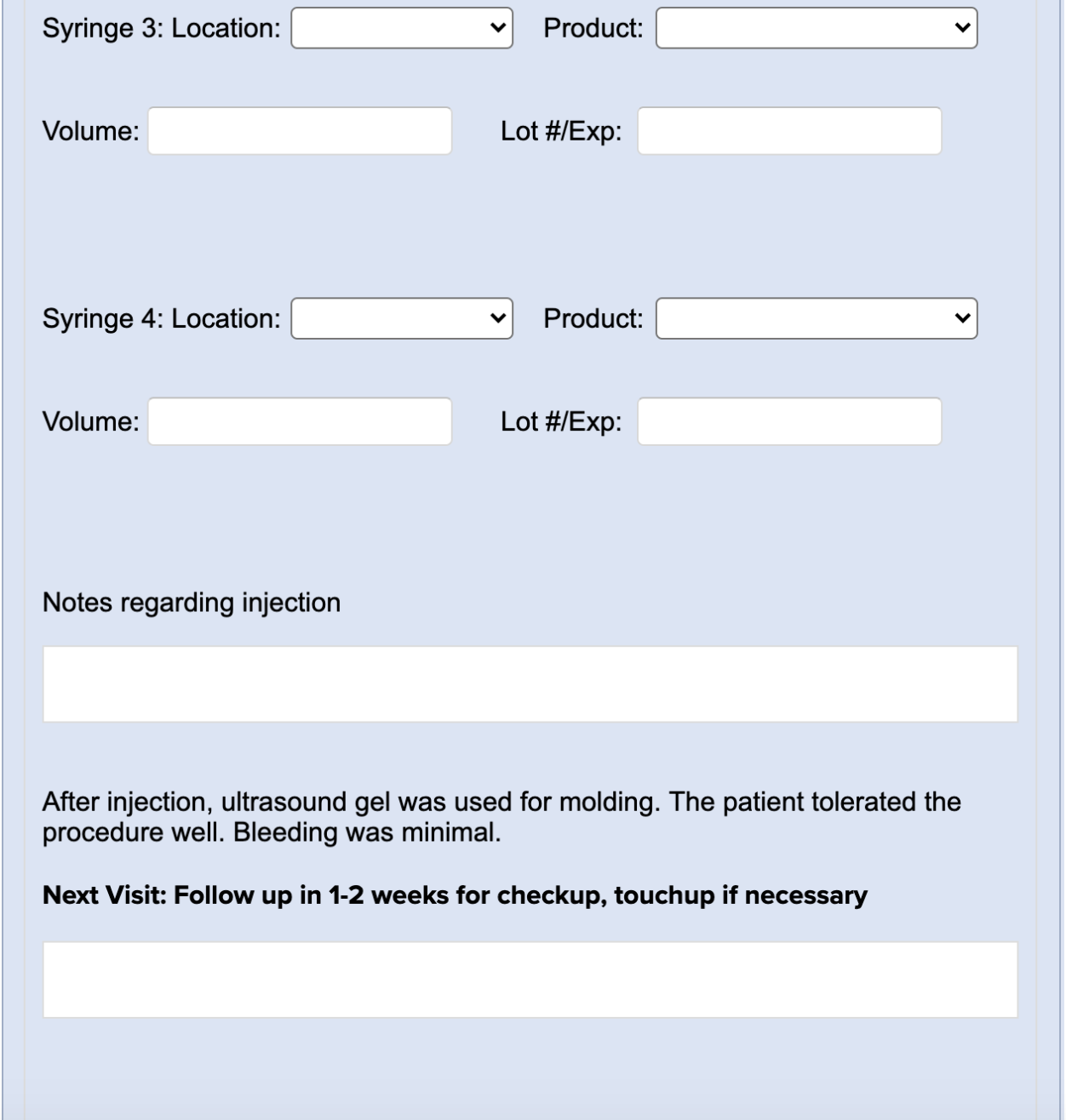
Toxin and Filler Treatment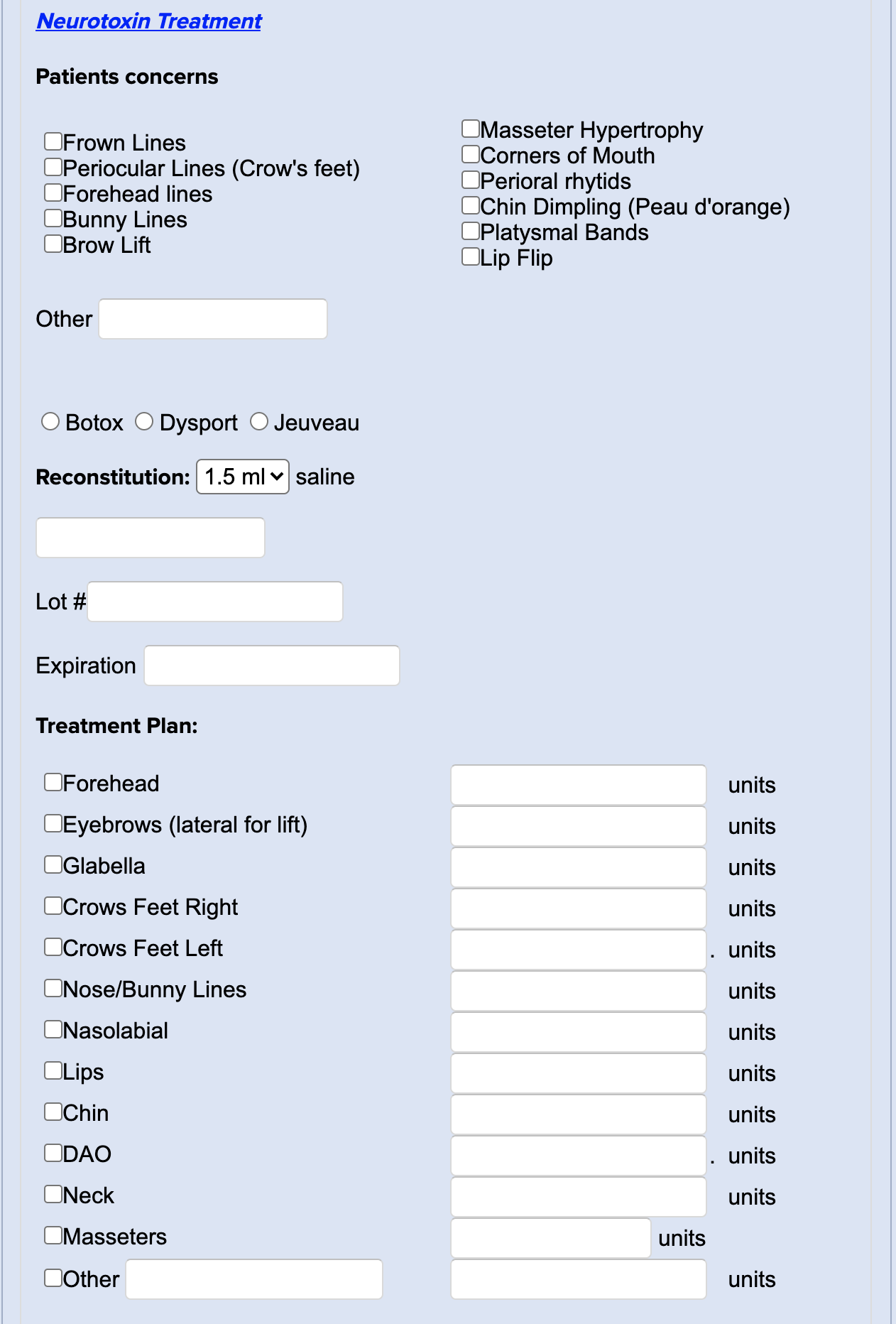
Upper Biepharoplasty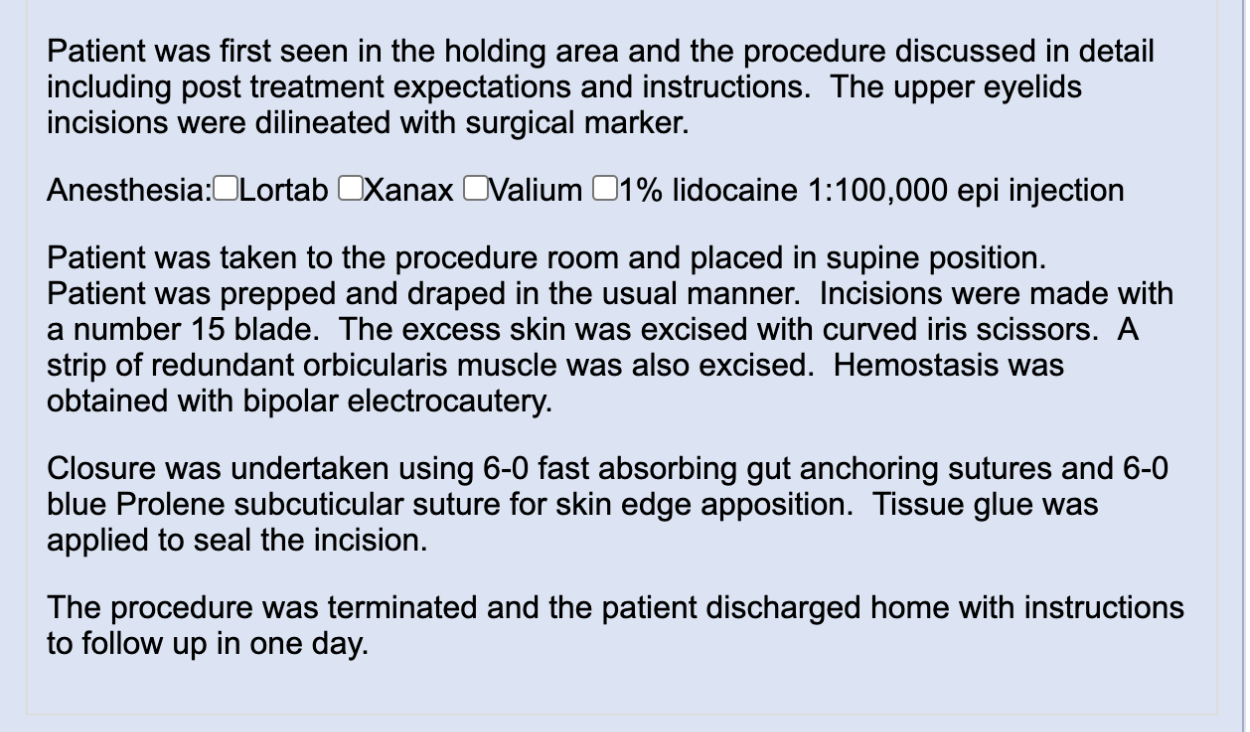
Weight Loss / Wellness Follow Up/Rx Refill/Injection
Medically cleared by ___(insert provider name)
Pt. presents for follow up visit for their weight loss & wellness program.
Evaluation completed by: ___Face to Face; ____Virtual Visit
Any side effects or issues from the current treatment program?___NO____YES;
If yes, please describe:
Any Medical history changes since last visit? ___No ___Yes
Are you on any new medications? ____ No ___ Yes. what meds? ____________
Repots no contraindications to today's tx,
BP:
Pulse:
Current weight:
Previous office visit weight:
Initial Weight:
LMP:
*If patient has been on phentermine for over 90 days, re-evaluate their progress and strategy and perform PMP check, then notify the medical director. Do not refill phentermine if patient has been on it for more than 90 days.
After careful review of the risks and benefits to all therapeutic options, the patient is approved for refill of the following:
____Testosterone Optimization: ____mg IM weekly
____Anastrozole ___mg tab weekly
____Estradiol ___mg
____Lipo Mino Mix (skinny shot) weekly
____Phentermine: ___37.5mg; ___15mg; ___#30; ___#90; ____ordered through Empower; ____dispensed on-site
____7-Keto DHEA/calcium/Phentermine ___15mg; ___30mg; ___37mg capsules: ____#; ____ordered through WellsRX
____Sermorelin ___15mg ____ordered today for home delivery; ___dispensed on site at dose;______mcg SC QPM
____Ipamorelin 15mg/Sermorelin ___15mg ____ordered today for home delivery; ___dispensed on site at dose;______mcg SC QPM
____Vitamin D 50,000 units weekly x 4 then monthly or oral equivalent
____OrthoMolecular DHEA ____mg daily
____Naltrexone: ___1.5mg; ___3mg; ___4.5mg daily; #____ dispensed on site today; #____ordered today for home delivery
____Thyroid Hormone: ___15mg; ___30mg; ___45mg; ___ 60mg; ___ 90mg
____T3 (Cytomel): ___5mcg; ___10mcg; ____ordered through WellsRx; ____dispensed on-site
____7-Keto DHEA: ___25mg; ___100mg; ____ordered through WellsRx; ____dispensed on-site
____Sarcotropin oral food; ___dispensed on site; ___ordered through WellsRx
____ECA Stack (ephedrine/caffeine/aspirin/chromium/B12); ___ordered through WellsRx
____Injectable Nutrients:______; ___ordered through WellsRx
____Hair Restoration therapies: ______; ___ordered through WellsRx
Plan:
___Start; ____Increase; _____Continue
1mg/ml Semaglutide with B12 (Empower / Hope). Sig:
___Inject 0.25 ml sq qw (0.25 mg Semaglutide)
___Inject 0.5 ml sq qw (0.5 mg Semaglutide)
5mg/ml Semaglutide with B12 (Empower / Hope). Sig:
___Inject 0.05 ml sq qw (0.25 mg Semaglutide)
___Inject 0.1 ml sq qw (0.5 mg Semaglutide)
___Inject 0.2 ml sq qw (1.0 mg Semaglutide)
___Inject 0.4 ml sq qw (2. 0 mg Semaglutide)
___Continue; ___ Start
___phentermine 37.5mg. take 1/2 tab days 1-2, then take 1 tab po qd x 30 days
___phentermine 37.5mg. take 1/2 tab qd x 30 days
___phentermine 37.5mg. take 1 tab po qd x 30 days
___tenuate 75 mg 1 po qd x 30days
Shots given today on site:
____B12 Vitamin
____LipoB Mino Mix (Lipo Fat burner)
___Biotin
____Vitamin D3 ____Glutathione
____Vitamin C ____B-Complex
____Testosterone
Location: ____Left Deltoid; ____Right Deltoid; ____Left Buttock;____Right buttock
Amount: __1_ml/mg;
Route: _x__IM; ____SC
___Semaglutide onsite injection
Location: ____Right abdomen; ____Left abdomen; ___
Amount: ___ units; ___ml/mg;
Route: _x_SC
_x__Follow Up: _x__30 day virtual; ___face to face at next visit with MD/PA/NP
Notes: