During a patient encounter, you may want to document their overall health including their vitals. You have the ability to do so in the Physical Exam section available as optional in every encounter note.
In this article you'll learn how to:
Access and Input Patient Vitals
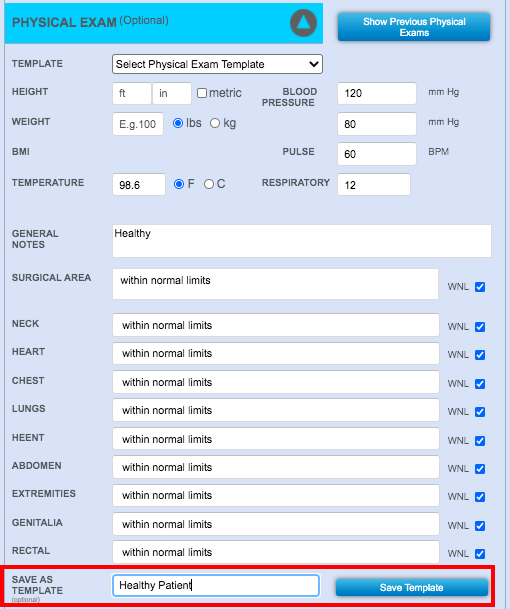
The physical exam section is always available for documenting patient vitals in both chart notes and op notes. To access, open a procedure or chart note and expand the Physical Exam section.
You can document the following vitals:
- Height and weight
- Blood pressure
- Pulse
- Temperature
- Respiratory
Along with it you can add general notes about the patient's condition as well as describe the condition of the following body areas:
- Targeted surgical area
- Neck
- Heart
- Chest
- Lungs
- HEENT (head, eyes, ears, nose, throat)
- Abdomen
- Extremities
- Genitalia
- Rectal
The inputs will be saved when the note is either Saved or Committed.
Check Previous Physical Exams
After you save the procedure or chart note, the vitals from the Physical Exam section will be available for viewing as a part of the note.
To access them, navigate to patient history and open the PDF of the appropriate chart or procedure note then navigate to the Physical Exam section.
You can also access all previous physical exam data by clicking Show Previous Physical Exams in the Physical Exam section within a procedure or chart note.

A summary of the historical data will display including all previous inputs.
Create a Physical Exam Template
The Physical Exam default section of the charting interface is not configurable. However it is possible to create and save physical exam templates for future use.
First input the preferred configurations relevant to the template you are creating and name your new template in the Save As Template field.
Your new template will be available in the Template pull down menu for future chart/op notes.
